Introduction: Good Sh*t
Dr Ben Mullish, a clinical scientist at Imperial College London, was running a trial of FMT in patients with C. diff infections. Ray was so unwell that Dr Mullish offered him the treatment. Heather understood that there are good and bad bugs and advised her husband to go ahead with it, but Ray was not having it. The idea of taking another human’s faeces was just too much for him, and he refused. Three days later, when he had deteroriated further despite the vancomycin, there was no other choice. Dr Mullish gained Ray’s consent for the trial and set to work on preparing for the transplant.
While a FMT might be a new idea to many of us today, the medical practice of faecal transplant is ancient, and it has been drunk as ‘yellow soup’ since the fourth century AD for the treatment of infective diarrhoea. In 1958 an innovative surgeon, Dr Ben Eiseman, administered faecal enemas to his patients in Denver, Colorado with severe recurrent C. diff infections. It was remarkably effective, but like all important medical discoveries, this intervention was largely ingnored at the time of its first report. More than half a century later, the Dutch gastroenterologist Josbert Keller and his team at Amsterdam Medical Centre randomised patients with recurrent C. diff into three groups. the first group received vancomycin, a wash-out of the colon using a strong laxative, and a faecal transplant. The second had vancomycin and the colonic wash-out, and the third just received vancomycin. The FMT group did so much better than the other two groups that the study had to be stopped early, as it was deemed unethical to continue; 93 per cent of patients who had an FMT got better, compared to only 31 per centwith the vancomycin alone, and 23 per cent with the vancomycin and wash-out.
The close evoluntionary relationship between our microbiome and the cells of our immune system may also explain why FMT appears to be so effective in reducing the immunological complications of bone marrow transplants used in the treatment of cancers of the blood such as leukaemia. Clinical trials of FMT that improve the diversity of the gut appear to reduce the chances of the immune system inadvertently attacking itself (this phenomenon is called ‘graft vs host disease’) and it improves the likelihood of this life-saving therapy working.
Although the female genital tract is dominated by bacteria, other microbes are also crucial to its health. Yeasts are obviously important; 75 per cent of women will have atleast one episode of candidiasis – or thrush – typically caused by the yeast C. albicans. Bacteria and yeasts in the vagina also coexist with viruses that help regulate these populations. For example, more than 400 phage have beeen identified for the thirty-nine Gardnerella strains of bacteria that are associated with the condition bacterial vaginosis, and almost 90 per cent of genomes of the vaginal and urinary Gardnerella strains contain atleast one genome from a phage embedded in their bacterial DNA. This means that phage play an extremely important role in the regulation of the vaginal microbiome and the maintenance of urogenital health. So no matter what Gwyneth Paltrow or any other celebrities say, if you have a vagina, do not steam it. You need your urogenital symbionts to keep you healthy.
There’s a powerful link between the make-up of an infant’s gut microbiota and the extent and duration of breastfeeding. For example, a study of babies in Thailand found that the abundance of Bifidobacteria was closely associated with how long babies had been breastfed for, and that babies fed with infant formula had significantly lower abundances of this species in the gut.
Stroke usually occurs in older people who have an ageing microbiome and less resilience to any injury in general, and multiple studies suggest that the severity of a stroke is greater in people who have a less diverse gut microbiome. For example, patients with stroke have increased abundances of Streptococcus, Lactobacillus and Escherichia and lower abundances of Eubacterium and Roseburia taxa in their gut, and these changes also co-relate with the severity of a stroke.
Losing our appetite when we’re ill might also promote metabolic changes in our bodies that keeps us healthy – for example, by limiting the nutrients available for pathogens that wish us harm. But some bacteria have learned to subvert this process for their own benefit, and they do it through the vagus nerve. Salmonella enterica is responsible for a quarter of all cases of diarrhoea, causing more than ninety-four million gastrointestinal infections each year.
We’ve made similar observations about the microbiome’s role in regulating our anxiety. Bacteria such as Bacteroides ovatus produce metabolites that break down dietary sources of tyrosine – which is found in foods such as soy, avocados, bananas and milk products. This metabolite interferes with a cell responsible for wrapping the axons of nerves in a type of fat. The fat allows the nerve cell to end its electrical signal along its arm-like axons, which connect with other nerve cells via a synapse to send signals.
Synaptic pruning happens when connections that are incorrect or no longer useful are destroyed and it is an important method for regulating this process. One hypothesis is that the development of our neurones is co-dependent on the gut microbiome, which undergoes parallel changes in its diversity and structure with the developing brain or to put it another way, the microbiome modifies the structure and function of emerging neural circuits, creating neurodiversity – and my dyslexia. The race is now on to define the precise mechanism through which this occurs.
It’s now recognised that many children with ASD also suffer from gastrointestinal symptoms ranging from constipation to diarrhoea, and that these might be under-reported.
A Chinese study of more than 773 children with ASD and 429 neurotypical children suggests that this might be more than mere coincidence. The researchers studied the dynamics of the gut microbiota across different ages, and found that the gut microbiome of children with ASD evolves in a way that is indeed influenced by diet and gut function. But this evolution is strikingly different from that of neurotypical children. Children with ASD have an immature gut microbiome, with less diversity, and the most important changes take place before the age of three. These observations in the microbiome closely associate with the severity of the behaviour change, sleep patterns and altered bowel function in the ASD group. Researchers were able to identify the children with ASD through the detection of bacteria Veillonella and Enterobacteriaceae, along with just seventeen microbial co-metabolites found in their stool, which differentiated them from the neurotypical children.
The severity of ASD also appeared to be significantly linked to the function of microbiome and bacterial pathways for tryptophan metabolism, which is relevant because it is used to make neurotransmitters. There’s more evidence to other metabolites created by gut bacteria that influence brain development. For example, bacteria in the gut putrefy proteins and one of the by-products of this process is a metabolite called p-Cresol. When this is given to mice, it selectively causes ASD behavioural symptoms and social behavioural deficits.
However, it also changes the composition of the gut microbiome, and when faeces from p-Cresol-fed mice is transplanted into control mice, they not only produce more p-Cresol, but also develop the same behavioural symptoms. Most interestimngly of all, when faeces from healthy control mice is transplanted back into p-Cresol-fed mice, their behaviour changes back to that of healthy mice.
These experiments don’t explain the role of the parenteral microbiome in the developmental conditions of neuro-diversity because it appears that a misdirected maternal immune sytem is important in the development of ASD.
Psychobiotics
Both Bacteroides fragilis and Lactobacillus reuteri have been observed to reverse some of the behavioural and gastrointestinal changes reported in animal models of Autism Spectrum Disorder, but these bacteria work in discretely different ways. for example, in a mouse model of ASD, L. reuteri rescues social behavioural deficits by working thropugh the vagus nerve to increase the amount of a pro-social hormone called oxytocin in the reward pathways of the brain. It also changes behaviour by creating a metabolite called tetrahydrobiopterin, which is a co-factor involved in the production of several neurotransmitters such as dopamine, serotonin and nitric oxide. It is also true that psychobiotics don’t simply work on any ASD-associated behaviours. For instance, they did not have any impact on hyperactivity behaviours because these are almost exclusively controlled by the host genetics of the animal.
Scientists can tell if you’re a day-worker or night-worker just by looking at your microbiome: an analysis of male security guards found that the Faecalibacterium genus abundance in the gut is a biomarker of day-shift work, Dorea longicatena and D. formicigenerans were significantly more abundant and important commensal bacteria of the human gut microbiota and is strongly associated with gut health.
So how do bacteria know what time of the day it is? Some bacteria, such as Bacteroides ovatus, possess their own internal clocks that do not rely on light. Instead their populations ‘oscillate’, based on environmental cues that come from diet and lifestyle.
In fact if you want to repair your nerves or your brain, eating less might also help: we’ve recently learned that intermittent fasting promotes nerve regrowth. This process relies on a metabolite called indole-3-propionic acid (IPA), which is produced by a specific bacteria called Clostridium sporogenes.
The GEM Line
An infinite number of factors can be grouped into three main forces: the genome, the exposome and the microbiome. These are the three forces that shape not only our risk of the disease, but also our experience of wellness and healthy ageing. Think of them as the axes of a three-dimensional graph on which we can plot the progress of our lives.
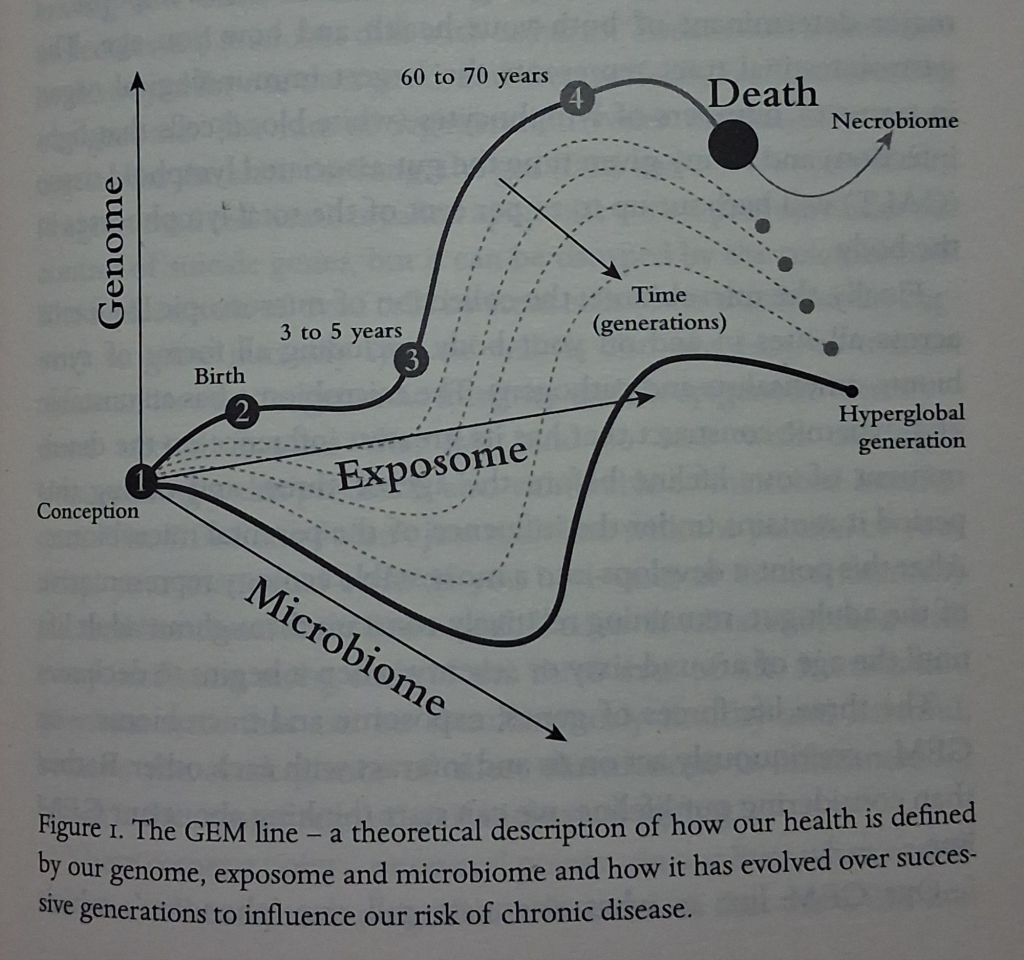
First is the genome – all the genetic information that makes up our bodies, and a major player in our ability to grow, function and age normally. For a minority of us, genetic mutations that we inherit will set our risk of getting a disease or experiencing an early death.
As you would expect, epigenetic gene modifications are also a major determinant of our risk of disease.
Second is the exposome – all the environmental forces that interact with our genome over the course of our lives. Your gut is your greatest environmental sensing organ, and it will taste, smell and ingest all of theee things. Which is why it has a complex anatomical and physiological architecture that allows it to function and to educate the innate immune response – a major determinant of both your health and how you age.
Third is the microbiome – a collection of microscopic life forms across all sites in and on your body, including all forms of symbionts, amensalists and pathogens. The microbiome has an unstable and dynamic construct hat has its greatest influence on the developmernt of our lifeline before the age of three, and during this period it remains under the influence of the parental microbiome.
The three life forces of genes, exposome and microbiome – or GEM – continuously act on us and interact with each other. Our GEM line is what scientists call our ‘phenome’, which describes all the measurable physical and chemical characteristics of the human body. It maintains internal stability while adjusting to changing external conditions and is able to adapt through growth and re-organisation. A hallmark of microbiome health is its resilience in dealing with fluctuations in the exposome or genome.
The GEM line allows us to conceive of how these three dominant forces influence our health over several generations. Young people, born during the age of hyperglobalisation that started in the 1990s with the rapid growth in economic, cultural and political globalisation, have experienced such a profound disruption to their microbiome and exposome that their risk of disorders of the immune system has been dramatically altered. Their trajectory is veery different from those of us born before this era, and this in turn bears little resemblance to someone who was born before the Second World War.
The gut-lung axis
The lower respiratory tract contains Streptococcus, Prevotella and Veillonella. In chronic infections of the lung these bacteria are often found in large clusters, called biofilms, which are much harder to physically cough up or remove and are more resistant to antibiotics.
The ageing microbiome
One of the most-enriched species in centenarians was Clostridium scindens, known to possesss a relatively rare enzyme called 7 alpha-dehydroxylase that’s needed to metabolise bile. Bile influences muscle-thinning, obesity, cardiovascular and cancer disease risk, and even the risk of neuroegenerative disease. Centenarians, it seems, have a distinct gut microbiome that is really good at generating unique bile acids, which limit inflammation in the gut.
The meta hypothesis
The first age refers to the maternal microbiome. Here, changes in the microbial orchestral signalling between a mother and her developing baby cause epigenetic modifications in developing organs and immune system. This sets the course for the whole of our lives, our brain development, behaviour, personality and risk for chronic diseases.
The second age takes place in the first three to five years of life; within this period, the most critical time is the first 100 days. If the seeding and dispersal of the developing microbiome are interupted, then the immune and metabolic systems can’t compete the programming of the systemic organ axes (brain, liver, lung, bone and heart). Our risk of disease changes once more, and our risk of allergy, atopy, autoimmune disease and mental-health problemss becomes more defined.
The third stage is the broadest and takes place between the ages of five and seventy. During this phase the ecological structure of the microbiome is relatively stable, but its functions can oscillate on an hourly and daily basis. Its chemical outputs are influenced by our diet, drug and xenommetabolite (non-host metabolite) interactions, which in turn determines our risk of diseases such as obesity and cancer. Its hardest to modify the microbiome for health benefits during this stage, which is at its most fixed.
The fourth stage takes place between the age of seventy (assuming we get that far) and our end of life. The microbiome is once more dynamic in its structure, influencing the balance between inflamm-ageing and immune-senescence. This in turn determines our cognitive decline, mobility and frality, the quality of the end of our life and our death.
Environmental contaminants also change the composition and functions of these bacteria in the gut and cause chronic diseases. Residents of Greater Baltimore, for example, have been exposed to unusually high levels of Chlorpyrifos, one of the most comon organophosphorous pesticides. It caused so many health problems that the city banned pesticides containing this agent in 2020. The damage inflicted on the gut and its microbiome by this toxin has been linked to high rates of obesity and diabetes among the city’s inhabitants.
The design of the buildings we live and work in influences not only our risk of exposure to pathogens, but also our chance of being exposed to symbiotic microbes that could be beneficial. This might be key to understanding our susceptibility to developing allergies. For example, house-dust microbiota are significantly different in rural and urban areas, with higher relative abundances of Ruminococcaceae, Lachnospiracea and Bacteroidaceae families in rural houses compared with urban houses. Children under five expoed to higher indoor concentrations of dust microbiome also experience an increased risk of lower respiratory-tract infections.
Urbanisation
The gut microbes of city dewellers have more metabolic pathways to degrade drugs and organic compounds, and they have lower abundances of rural Prevotella spp. and fermentative Clostridiales, with Enterobacteriaceae and Bacteroides spp. useful for metabolising a diverse diet. But the design of our cities also influences the bacteria that we are exposed to.
It’s likely that air pollution is also contributing to changes in the composition and function of the human gut micrbiome. Long-term exposure to micro-scale particulate matter, nitrogen dioxide, ozone and nitrogen oxides is asssociated with a greater risk for obesity, glucose dysregulation and type II diabetes. We breathe in ultra-fine pollutants and thtese make their way into our blood circulation and to our gut. A study in California demonstrated that exposure to ozone for twenty-four hours was associated with reduced gut microbial diversity and increased abundances of Bacteroides caecimuris. Nitrogen-dioxide exposure was also associayed with changes in gut ecology with the loss of a number of taxa.
Modern family
How often you interact with family will also play a role in defining the bugs you share. For example, going home for thanksgiving or religious holidays is an important method of reconnecting with the family microbiome. Researchers performed a metataxanomic analysis of fecal samples collected on 23 and 27 December from a group of twenty-eight healthy volunteers celebrating Christmas. They find two distinct microbial-biomarkers signatures: those who had decided to see only their immeadiate family over the Christmas season, and those who’d visited both their own family and their in-laws. Participants visiting in-laws demonstrated a decrease in all Ruminococcus species, which may mean that they were not made to eat Brusels sprouts. Several attempts have now been made to study the dynamics of family microbiome networks. The Fiji Community Microbiome Project (FijiCOMP) explored the role of bacterial transmission in human populations in 287 people living in five agrarian villages in the Fiji Islands. Within this small community of individuals with homogenous living environments, diets and microbiomes, bacterial DNA alone could be used to accurately predict certain initimately linked pairs of individuals. Strong transmission patterns were also found within households. Women were more likely than men to harbour strains that were closely related to those found in family members and social contacts.
Resistance is futile
The humanitarian response to recent conflicts in the Middle East has been dominated by their local environmental microbes and pathogens. After the Allied invasion of Iraq in 2003, US military surgeons began reporting on a multi-drug-resistant bacterium they called ‘Iraqibacter’. The actual organism was Acinetobacter baumannii, a bacterium that only served to increase the true horror of wounds because they became infected or didn’t heal. This was far from the only resistant organism. In Afghanistan, Allied forces had to deal with the high rates of aggressive multi-drug-resistant bacteria like Panton-Valentine leukocidin (PVL) producing Staphylococcus aureus, which caused terrible soft tissue infections. As if war were not bad enough, modern-combat medics must now deal with antibiotic stewardship and multi-drug resistance.
But combat doesn’t only influence our relationship with pathogens – it also mutates our commensal and amensalist microbes, and this is just as important. Gulf War syndrome is a chronic and multi-symtomatic disorder affecting military veterans of the 1990-91 Persian Gulf War. A wide range of acute and chronic symptoms have been linked to it, including fatigue, muscle pain, cognitive decline, insomnia, rashes and diarrhoea – all symptoms that are typically seen when the immune system isn’t functioning. While the cause of this condition is debated, it’s thought to be related to exposure to pills containing pyridostigmine bromide, a pre-treatment for nerve agents, pesticides or chemicals from oil wells, among other compounds. These agents not only perturb the gut microbiome, but also injure the gut barrier, causing a systemic inflammatory response in animal models.
A proportion of veteran soldiers suffering from this conditionhave gastrointestinal symptoms, and the type of microbes in their gut varies from thpose who don’t have symptoms. Specifically, they have greater abundances of Bacteroides, Actinobacteria, Euryarchaeota and Proteobacteria, as well as higher abundances of the families Bacteroidaceae, Erysipelotrichaceae and Bifidobacteriaceae. These bacteria are linked to increased levels of inflammation in the blood and worsening of other symptoms. This could, of course, be an effect rather than a cause, but the microbiome is implicated.
Of the 15,000 veterans surveyed in one study, nearly 50 per cent were overweight and about 30 per cent were obese. Obese veterans were more prone to developing other chronic health conditions such as post-traumatic strtess disorder (PTSD). The gut microbiome is initimately linked to obesity and mental health through the gut-brain axis, and its plausible that it is playing an indirect role in causing the symptoms of Gulf War Syndrome.
Climate Conflict
The fact that Mongol fighters achieved casualty rates comparable to those of modern mechanised combat has nothing to do with swords or gunpowder. In the conflicts of old, the real harm was caused by plagues and pathogenic microbes, which decimated armies, civilian populations and refugees. By 1550 approximately twenty-four million Azrecs were killed, with 1.5 million in the Mayan states and eight million Incas. Influenza, smallpox, measles and mumps killed millions of these people, and researchers now believe that ‘cocolitzli’ – a thyphoid-like enteric fever – as largely responsible for the majority of deaths that finally led to the collapse of the Aztec empire.
You can take your pick from a number of refugee camps to tell this story: Kakuma in Kenya, Za’atari in Jordan or Um Rakuba in Sudan. All host vulnerable people at the mercy of pathogens and disease vectors, and many of these camps are devasted by COVID-19.
The home front
In March 1945, the British War Cabinet had to deal with a nation facing serious food shortages and a rationing crisis. With a prospective deficit of 1,800,000 tons of meat, something had to be done. farmers were encouraged to adopt the newly discovered antibiotic prophylactic strategies to prevent disease, reduce costs, maintain production, preserve food and minimise economic risk. Pullorum disease in poultry, for example, is caused by the bacterium Salmonella pullorum. It is vertically transmitted and typically affects young chicks and has a high mortality rate. Before the war, farmers had to resort to scrubbing hatching trays and eggs with hot lye, or using carbolic acid or chlorinated lime. Eggs and hatching chicks were even fumigated with oncogenic and highly toxic products, such as formaldehyde or potassium permanganate. In 1948, Merick’s sulfaquinxaline became the first antibiotic to be officially licensed for routine inclusion in poultry feeds against the protozoa coccidiosis.
As early as 1946 scientists observed that antibiotics triggered more efficient growth in poultry and swine when they were fed the mycelia of the fungi Streptomyces aureofaciens that contained chlorotetracycline antibiotic.
The resistome
A major driver for antibiotic resistance comes from the environmemt and ‘Big Ag’. Of course we also give a lot of antibiotics to humans. A recent analysis from the Department of Global Health at the University of Washington analysed worldwide antibiotic prescribing rates. It found that global antibiotic consumption, expressed in defined daily doses (DDD), increased by 65 per cent between 2000 and 2015 to somewhere between 21.1 and 34.8 billion DDDs, and this increase was much higher in low- and middle-income countries. As a result of this orgy of prescribing, the UK now spends about £1 billion each year trying to treat the most common resistant bacteria like E .coli, Klebsiella pneumoniae, Enterococcus faecium, Pseudomonas aeruginosa and Methicillin resistant Staphylococcus aureus (MRSA) – all pathogens that no longer respond to the last line of antibiotic defences.
Patancheru is an industrial zone twenty miles outside Hyderabad in central India, a region with diverse waterways and lakes. The irony is that the patients treated in clincs and hospitals in this region require larger doses of antibiotics for treatment, sometimes incorrectly prescribed for the chronic inflammatory conditions that are caused by antibiotic contamination, such as eczema and asthma, and the hospitals where they are prescribed return these antibiotic resistant genes back to the rivers. Multiple experiments have identified that untreated hospital wastewater from acrosss the world strongly selects for multi-resistant E.coli.
Using metagenomic strategies, we’re now able to study antibiotic resistance genes across poulations to get a sense of the size of the problem. The International Metagenomics and Metadesign of Subways and Urban Biomes (MetaSUB) demonstrated that the number and type of antibiotic resistance genes found in microbiomes in cities vary widely. Some cities, like Bogota, have fifteen to twenty times more resistance genes than European cities such as Stockholm, which, given its progressive approach to managing this problem, has a low density. As well as reflecting varying antibiotic policy, the MetaSUB findings can be put down to differences in urban geography or to the variation in the baseline microbiome.
The data on the gut resistome tell us something profound about the evolution of the human microbiome, which has been transformed in just seventy years. In 1961, Waksman pointed out that naturally occurrimg antibiotic molecules made by some bacteria may have important signalling roles because they can influence how genes are transcribed in target bacteria.
Antibiotics can also reach the infant via the breastmilk. Several studies have found associations between maternal antibiotic use and an increased risk of asthma, wheezing, eczema and atopic dermatitis in babies, although the link with food allergy seems to be less strong. Antibiotic treatment in the first week of life is also independently associatted with an increasd risk of wheezing and infantile colic, and exposure to antibiotiocs during the first year of life has been strongly asociated with childhood asthma, allergies and changes in infant birth weight, even after adjusting for familial factors.
While antibiotics will have the biggest effect on our microbiome in infancy, taking them as adults can also affect our risk of developing some chronic diseases. UK researchers studied 22,677 patients with rheumatoid arthritis, an autoimmune disease that typically causes painful and debilitating swelling of the joints. They compared this group to 90,013 people without the condition, burt of comparable age and sex, and looked back ten years before the onset of the rheumatoid diagnosis. Patients who’d beeen given antibiotics during this time were 60 per cent more likely to develop the condition than those who hadn’t, and this also correlated to the dose or frequency of antibiotic prescriptions. Interestingly, both antifungal and antiviral prescriptions were also associated with an increased risk of getting this disease. The second major factor is the type of antibiotic. Finally, the frequency with which children are given antibiotics also matters.
Globally in 2021 the most profitable drug was a medicine called Humira, an antibody used in the treatment of auto-immune diseases like rheumatoid arthritis and inflammatory bowel disease; it made the pharmaceutical giant AbbVie approximately US $120 billion. Both of these medicines are designed simply to keep these diseases in a very profitable remission.
The MetaCardis study is a cross-sectional analysis of 2,173 European residents with metbolic syndrome. Through it, we’ve discovered that the impact of ppolypharmacy on the gut microbiome is so great that it can exceed changes caused by the underlying disease. But this isn’t always bad; the study also demonstrated that there are additive effects of multiple drugs, which can sometimes shift the microbiome towards a more protective structure and function.
After cholesterol-lowering drugs, the next most likely to be dumped on to the repeat-prescription list is a class of medication called ‘proton pump inhibitors’- regular users have a slightly increased risk of Clostridium difficile inmfection, and gastrointestinal side-effects are commonly reported. But these drugs are also associated with an increased risk of gastric cancer, inflammatory bowel disease, chronic kidney disease, stroke and even dementia.
Many of the more routine drugs we take to manage our chronic disease have an indirect influence on our microbiome, and we’re slowly beginning to unravel the complexity of these interactions. the severity of the COVID-19 infection was also associated with over-abundances of bacteria such as Coprobacillus, Clostridium ramosum and C. hathewayi that are commonly found in the gut and mouth. In reality, thre microbiome regulates food metabolism, host energy control, fat accumulation, and gut-barrier integrity through shared molecular functions. And there is evidence that some strains play a more important part in this process than others. For example, obesity is associated with lower intestinal abundances of mutualistic bacteria such as Akkermansia muciniphilia, which improves gut-barrier function and insulin sensitivity.
Syndrome X
Karelia is a staggeringly beautiful wooded region in northern Europe that is politically significant to Finland, Russia, and Sweden. It has a turbulent history. Children growing up on the Finnish side have an incidence of type I diabetes that is five to six times greater than those growing up on the neighbouring Russian side, and they also have a higher risk of allergies. Bacteroides species dominate in Finns and Estonians. These endotoxins, produced by Bacteroides dorei, are structurally different from those of Escherichia coli, which was the predominant endotoxin in the Russian gut.
A team of Chinese scientists looked at the faeces of forty-three people with NAFLD alongside those of forty-eight healthy people, and found significantly greater abundances of a strain of an alcohol-producing bacterium callled Klebseilla pneumoniae in the patients with NAFLD compared to the healthy group. When these strains were given to mice as part of an FMT study, the mice also developed NAFLD. If these baceria were eliminated from the FMT before it was given, the mice did not develop the disease.
Studies such as this one in Bangladeshi and Malawian children have demonstrated that the gut microbiome is slower to mature in malnourished states. They developed what they called a microbiota-directed complementary food (MDCF), specifically designed to meet the requirements of the microbiome in malnourished children. The results showed a moderate but significant improvement in the children’s weight-for-length and weight-for-age scores when compared to the control diet.
One of the most popular diets to treat inflammation of the gut, known as the low fermentable oligosaccharide, disaccharide, monosaccharide and polyol diet, or FODMAP. Excluding these fibres reduces the amount of gas produced – easing the symptoms of bloating. For example, the diet typically leads to a reduction in the relative abundance of Bifidobacteria, Faecalibacterium prausnitzii and Clostridium cluster IV and there’s even suggestion that bacteria may predict treatment response.
In some countries, such as the US, medicinal probiotics are oftem referred to as Live Biotherapeutic Products (LBPs) by regulators, in a bid to describe their roles when it comes to treating diseases more accurately. The most used probiotic genera include Lactobacillus, Bifidobacterium, Streptococcus, Enterococcus, Escherichia, Bacillus and the yeast Saccharomyces. Although they may share some common functions, each probiotic species is actually a discrete entity that will interact differently with our gut.
Source & Credit; Dark Matter – Dr James Kinross (2023)
Dr James Kinross is a senior lecturer in colorectal surgery, a consultant surgeon at Imperial College London and a visiting professor at the Royal College of Surgeons of Ireland. He leads a research team defining how microbiome causes cancer and other chronic diseases of the gut. Dark Matter is his first book.
