The Marburg virus disease (MVD) made its clinical appearance in humans in 1967 in Marburg, Frankfurt in Germany and then in Belgrade, Serbia. 31 deaths and 7 infections. Data show that 25 of them were lab workers; 5 were medical personnel and 1 was a family member. In 2023, Tanzania had a case fatality rate of 67% and Equatorial Guinea had the case fatality rate at 88%. There’s a lot of panic about the health situation of the population in Rwanda with the authorities working collaboratively to curb the spread and follow a strict protocol to enforce control measures.
There was also fear at some point that the Soviet Union would use this contagious microbe as a bio-weapon as early as 1991. This disease is also transmissible on contact with a dead body during an autopsy. Rousettus aegyptiacus bats are the natural hosts for the Marburg virus. The African green monkeys (Cercopithecus aethiops) imported from Uganda were the source of infection for humans during the first MVD outbreak. This was while research was conducted on these infected monkeys along the Lake Victoria. Research teams would come in contact with the exposed bodily fluids, that eventually led to the first human outbreak. The most common transmission would be a needle-stick injury in this case. Among the local common folk, the spread would occur through infected animals. The incubation period is approximately 2-21 days. Initially, it begins with high fever, severe headache and severe malaise. Muscle aches and pains are a common feature. On the third day, severe watery diarrhoea, abdominal pain and cramps, nausea and vomiting follow. This disease is sometimes confused with other endemic and tropical diseases like malaria. A non-itchy rash has been reported in patients between 2-7 days after the onset of symptoms. On the 5th day of the disease, patients can develop haemorrhaging manifestations, which includes fresh blood in vomitus and faeces, bleeding from the nose, gums and the vagina. Bleeding could also occur at the sites of the blood collection. The CNS being affected can result in confusion, irritability and aggression. The fatality occurs between the 8th and the 9th day which is preceded by severe blood loss and shock. Diagnosis is performed either by: antibody-capture enzyme-linked immunosorbent assay (ELISA), antigen-capture detection tests, reverse transcriptase polymerase chain reaction (RT-PCR) assay, virus isolation by cell culture in maximum containment laboratories.
Reducing the risk includes avoiding contact with infected animals, avoiding close and direct contact with infectious patients, avoiding recently deceased bodies after an infection from the virus, rapid act-fast containment measures. Taking extra care in the healthcare environment by wearing protective equipment and maintaining one’s hygiene after an infected patient contact is essential. There’s no available treatment in 2024 for this disease.
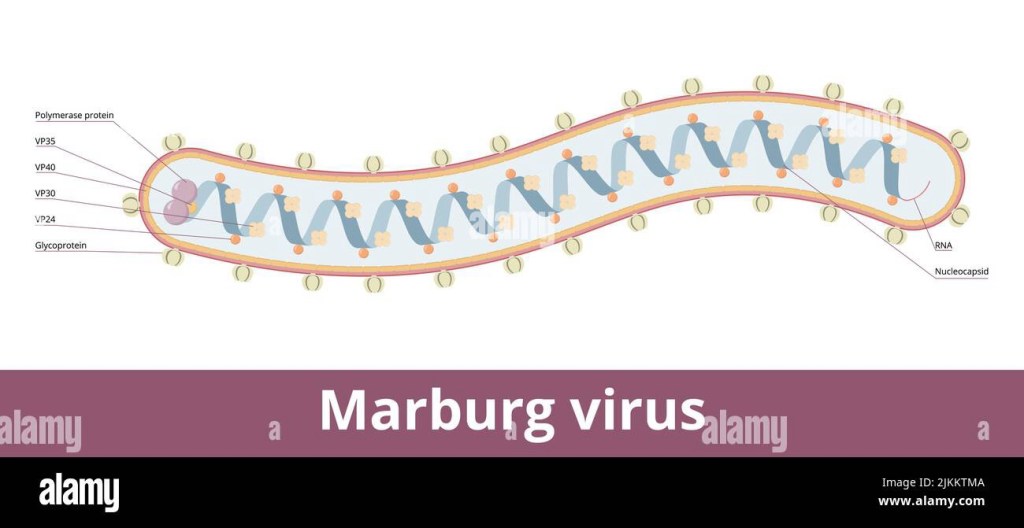
Sources: https://www.alamy.com/marburg-virushemorrhagic-fever-virus-of-the-filoviridae-family-virion-visualization-includes-glycoproteins-rna-and-nucleocapsid-image476794874.html?imageid=D590E19D-5A1B-44A0-9C6B-CA43E7ACE703&p=1874388&pn=1&searchId=1ffce49d84ec66eb66b34604030fb027&searchtype=0, https://www.who.int/news-room/fact-sheets/detail/marburg-virus-disease
