The strikes in a doctor’s eyes and mind are needed. But, the patients must be duly informed and treated.
There a few key public figures alongside the public who disagree with wanting to increase the pays.
“It’s damaging to the doctors and patients. It means somebody will die even if it’s a matter of one or two days after the strike has started.”
-Professor Robert Winston
The doctor has resigned from the British Medical Association after 60 years of membership.
Lord Ara Dazi who was a former Health Secretary and a Surgeon, led an independent investigation into the NHS of England last year. He says that the strikes are unjustifiable and that the resident doctors will lose the public’s trust. However, the criticism received by the public didn’t change and the BMA and the doctors are continuing to strike against the pressing issues.
The investigation has found the NHS to be in a “critical condition”, with surging waiting times, care quality issues in some areas, a lack of staff and funding for primary care services, and falling productivity rates resulting from poor patient flow. The review cites four interrelated drivers of these performance issues: (1) austerity in funding and capital starvation; (2) the impact of the pandemic, with more appointments cancelled than in other health system; (3) a lack of patient voice and staff engagement, including the effects of staff burnout; and (4) management structures, systems and the disruption caused by past reforms.
The BMA is calling for action in four key areas:
- Pay and debt: reversing years of real-terms pay erosion is the first step in rebuilding good faith, showing doctors they are valued and retaining them. A failure to do so will mean that doctors will continue to leave for better paid jobs elsewhere.
- Working conditions: working conditions need to make doctors want to stay, not push them out of the door, but too frequently they are uncaring, uncomfortable and unsafe.
Governments, health systems and employers must act to reduce workload pressures, improve work-life balance, expand access to basic facilities and services and stamp out harassment and abuse. - Diversity and inclusion: the NHS is fortunate to have a workforce that has become more diverse over time. To keep this diverse workforce, action needs to be taken to end discrimination and support those with additional needs to contribute to their potential.
- Development and support: in the context of relentlessly pressured environments, staff are afforded less and less time for learning and development. To better retain staff, employers need to ensure that doctors are able to practise in roles that make the most of their skills and experience, with the support to develop and progress personally and professionally.
Several deaths have been linked to these strikes where patients were unable to receive the care they need. Sir Jim Mackey has written a letter to the NHS bosses stating that this time you cannot cancel many operations and that you need to keep as much care going as possible, and only cancel operations if there is no doctors readily available to perform it. Whereas in previous strikes, it’s called Christmas Day Level of Service; when it’s the A&E alone that keeps running including any urgent critical care and all other routine care is called off. The British Medical Association have written back to Mackey and accused him of putting patients at risk. The NHS Confederation, however, have responded back to Mackey positively and agreeably sharing the same sentiments ambition-wise. Resident doctors have had the biggest pay rise in the public sector, Nurses are furious and have said it to be ‘grotesque’ even the Royal College of Nurses have admitted to the fact that the doctors have got the largest pay rise when nurses didn’t. Of course, this would also mean that the Health Secretary Wes Streeting would be forced to comply with whatever pay the nurses strike for and it will affect the Labour Party elections this year. He has agreed to improving the conditions of doctors as opposed to the further increase in the pay.
Furthermore, is IA by doctors ever ethically defendable?
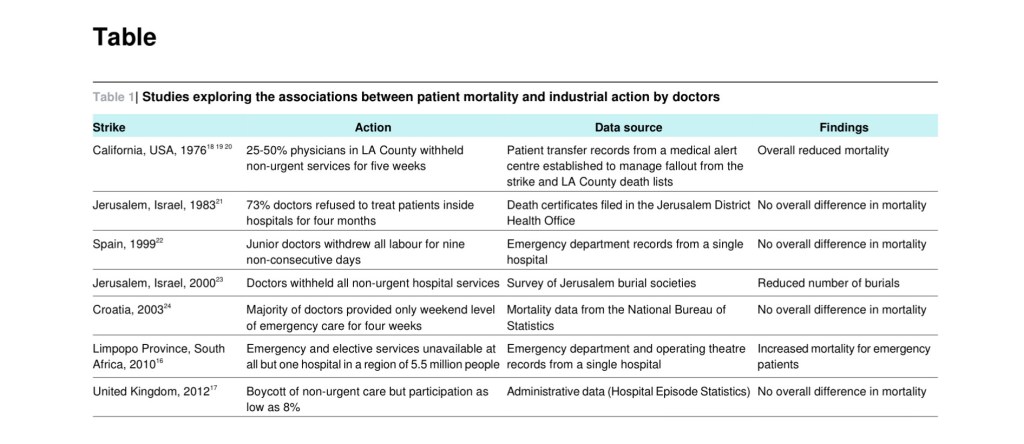
Industrial action (IA) by healthcare workers is not unknown, occurs in a wide range of healthcare systems and societies, and has complex ethical implications. For some, doctors striking amounts to exploitation of the suffering of patients for personal gain by the professionals in whom society puts more trust and is therefore indefensible in any circumstances. However, the moral legitimacy of strike action is generally accepted, especially if the actions of the employees only negatively impact the employers. In practice, for public servants in particular, IA will invariably impact third parties. Others, including doctors and other healthcare workers are not barred from IA but are often considered to be special moral cases due to the nature and obligation of their work. As these obligations are committed to freely, and are of such importance to society, once undertaken some feel strike action or withdrawal of labour at excessively short notice, constitutes a definitive moral wrong. This special contract endows privileges and responsibilities and doctors therefore have a ‘moral obligation’ to set an example to the rest of society and accept a greater degree of self-sacrifice while being rewarded a sense of pride and moral satisfaction.
To sustain an absolute moral objection to IA by doctors based on a breach of an unconditional special trust requires an acceptance that once a person becomes a doctor they are obliged to work under any conditions, at any time, with any number of patients. Such a conception of doctors’ duty may have been defendable when medical care consisted of little more than a caring attitude from a paternalistic authority figure who was free to choose their own patients. But in the modern context this simplistic notion of a doctor’s duty appears naïve.
Is IA by junior doctors ethical?
Understandable action is not the same as morally acceptable action, especially where patient care is involved. To help guide doctors in such circumstances ethical criteria have previously suggested, but all from different times and contexts. From the perspective of the current situation we conclude that for doctor IA to be morally permissible:
- All patients must still have access to emergency care.
- Maintenance of patient wellbeing must be a goal.
- Strikers must feel that all possible other forms of communication have failed.
Mark Toynbee et al make exactly that point: it would be unconventional at best to argue ‘that once a person becomes a doctor they are obliged to work under any conditions, at any time, with any number of patients’.’ What is lacking in the current debate, as in others for strikes in the past, are frameworks for assessing the ethics of doctors’ strikes which take that reduction seriously.
Resident doctors are demanding a 29% pay rise, and the BMA and the NHS have renamed ‘junior doctors’ to ‘resident doctors.’ Resident doctors who have graduated from medical school and have been working in the NHS for up-to a decade. There are two different measures of inflation; one is called retail price index (RPI), the second is called consumer price index (CPI). The Retail Price Index (RPI) is a measure of inflation, which in turn is the rate at which prices for goods and services are rising. CPI stands for consumer price index, an average of several consumer goods and services that are used to give an indication of inflation. The RPI factors for a doctor are student loans, mortgages and housing costs and the CPI is favoured by statisticians and government officials, and is seen as a reliable indicator inflation. Students graduate with £100,000 of student debt.
The first step is to acknowledge the independence in principle of two important ethical questions. The first is that of how doctors should conduct their work as doctors: of what moral standards apply to them while acting as medical professionals. The second is that of for what reasons and to what extent they may temporarily suspend that work, as they do when obeying a full or partial strike.
On the framework suggested, it also matters first how and by whom strikes are coordinated, and second how effectively the details of and justifications for industrial action are communicated.
The question of whether the recent strikes have been legitimately organised seems straightforward enough to affirmatively answer. The coordinating body is the BMA, the trade union and professional association for British doctors. The BMA first balloted junior doctors in England on a proposal of industrial action in November 2015, with 98% of those voting stating that they were ‘prepared to take part in industrial action including trike action’. The leading industrial relations barrister, John Hendy, rebuffed a suggestion by a National Health Service (NHS) Trust that participating in a strike might be nevertheless unlawful. 15
To keep updated;
https://x.com/bma_gp/status/1955593211323502786?s=46
https://www.bbc.com/news/articles/c5yl7qq1l9xo
https://youtu.be/AKfhIGIVtwc?si=T_KwAnHjzr8ABbap
https://www.bbc.com/news/articles/c4ge4905eq7o
Source:
Times Radio-Why the doctors are striking? The Story
https://www.jstor.org/stable/44014332?read-now=1&seq=4#page_scan_tab_contents
https://www.jstor.org/stable/44605993?read-now=1&seq=1#page_scan_tab_contents
https://www.jstor.org/stable/26523547?read-now=1&seq=1#page_scan_tab_contents
https://www.ig.com/uk/glossary-trading-terms/rpi-definition
https://www.ig.com/uk/glossary-trading-terms/cpi-definition
