It is a significant observation that neurosurgery flourished only in those centers of general surgical renown where neurology was already preeminent. In New York the foundations of the specialty were laid by such distinguished neurologists as William Hammond, Edward Seguin, Charles Dana, Allen Starr, Bernard Sachs, and Graeme Hammond, working with a notable group of general surgeons, including Robert Abbe, Charles McBurney, Andrew McCosh, and Frank Hartley. That this city had early attracted an able and brilliant group of neurologists is attested by the fact that among their number were seven of the founders of the American Neurological Society and sixteen of the original thirty-five members of that organization.
Prior to discussing the observations of these men, however, it is pertinent to go back a little further and to consider some fundamental advances which had then only recently been made in the knowledge of the anatomy and physiology of the central nervous system.
The new subjects of cerebral localization and spinal physiology had only begun to unfold.
Before it was recognized that definite functions are served by certain cerebral areas, the brain had been considered as a unit, functioning like any of the visceral organs.
The principle of cerebral localization, first suggested by Gall (37) in 1809, and given more definite form in Bouil-laud’s (16, 17) claim (1825-1848) that derangement of speech follows a lesion in the anterior lobe, had been frequently challenged. This view had been advocated also by Marc Dax 28) in 1836, but his observations seem to have attracted little attention until their presentation by his son, G. Dax (28), in a Memoir published in 1864. Meantime the debate had been vigorously waged at a meeting of the Société d’Anthropologie in 1861. Gratiolet (41), representing the opponents of the theory, declared:
“I do not hesitate to conclude that all schemes of localization hitherto proposed are without foundation. These are doubtless great efforts, titanic efforts, but when from the top of such a Babel we attempt to seize on divine truth, the edifice crumbles.”
On the other side of the argument, Auburtin (11), faithful disciple of Bouillaud, cited cases to prove his point, maintaining that, if instances of injury to the anterior lobes were discovered in which speech was not affected, these served only to prove that the part of the lobe concerned with speech was not involved. Going still further, he challenged Gratiolet to a definite test.
There was at that time on the service of Professor Broca (18) at the Hospital for Incurables (Bicêtre) a patient who had lost his articulate speech some years before. Auburtin agreed to renounce the doctrine of Bouillaud if autopsy failed to demonstrate a lesion in the anterior lobes of this patient. Broca, who previously had been hesitant to accept the doctrine of Bouillaud, agreed to the challenge, and when at necropsy a lesion was demonstrated in the third left frontal convolution, he became a most ardent advocate of the doctrine. Confirmatory evidence was obtained at a second autopsy, performed shortly thereafter, permitting a still more definite localization of the speech center in the posterior part of the third left frontal convolution.
In England, Hughlings Jackson (50) had become interested in the problem of cerebral localization, and his astute clinical and pathological deductions on the anatomical significance of localized seizures paved the way for galvanic stimulation of the cortex in lower animals by Fritsch and Hitzig (35) in 1870, and for Ferrier’s (32) faradic stimulation of the motor area in monkeys in 1874 to prove that the motor centers were to be found in the ascending convolution.
These views were sub-sequently brilliantly advanced by Horsley (47), Schaefer (47), and Beevor (13). Turck (78), in 1851, had demonstrated the relation of descending degeneration in the cord to cerebral involvement, and some six years later he described the essential lesion of tabes dorsalis as a sclerosis of the dorsal columns. In 1861 Brown-Séquard (19, 20, 21) pointed out the anatomical significance of a lesion affecting one-half of the spinal cord, and between 1873 and 1876 Flechsig (33) published a series of papers on the diseases of the spinal cord based on his own embryological and anatomical studies.
Hardly fifty years before this, the third edition of Wistar’s (81) Anatomy (the first American anatomy), dated 1825, had contained only the following description of the convolutions of the human brain: “The surface of the brain resembles that of the small intestine, or of a convoluted cylindrical tube; it is therefore said to be convoluted. The fissures between the convolutions do not extend very deep into the substance of the brain.”
While knowledge of the cerebral and spinal functions evolved, Lister, at the Royal Infirmary in Glasgow, had made his great contribution to antiseptic surgery, so that the fatal infections which had previously followed almost any cerebral or spinal operation, could be avoided and the surgical procedures pursued with a reasonable degree of safety. Thus, thanks to the neurologists’ advancement of cerebral and spinal localization, and the surgeons’ development of antisepsis, the achievements of neurosurgery were made possible.
I wish that time permitted me to present more fully the biographical data on the distinguished neurologists and general surgeons who contributed so brilliantly to the progress of neurology and neurosurgery in New York. I shall offer only a few remarks on the two earliest and most eminent neurologists, who laid the foundations for their specialty in this city so firmly and broadly that those who succeeded them were able to carry their work to a high degree of perfection. I refer to William Hammond (43) and Edward Seguin (68, 69, 70, 71, 72) who in succession occupied the chair of neurology at the College of Physicians and Surgeons of Columbia University.
William Hammond of New York, one of the founders of the American Neurological Society, had been Surgeon General of the Army in which he instituted many reforms. He wrote a Medical and Surgical History of the War of the Rebellion and established the Army Medical Museum. He insisted on adequate housing for the sick and wounded, set up a permanent army hospital, now the Walter Reed Hospital in Washington, and founded the Army Medical School and Library. On his return to New York from his military duties, he was invited to join the faculty of the College of Physicians and Surgeons as Professor of Neurology His textbook on Diseases of the Nervous System, in the writing of which his son, Graeme Hammond, collaborated, played an important role in furthering the study of neurology. This book, first published in 1876, had gone through nine editions by 1891, and had been translated into French, Italian, and Spanish.
Hammond was followed by Edward Seguin, one of the most brilliant and distinguished New York neurologists of the period. Seguin was graduated from the College of Physicians and Surgeons at the age of nineteen and subsequently became Professor of Diseases of the Mind and Nervous System in that institution. After the Civil War he studied in Paris under Ronvier, Charcot, and Brown-Squard. So distinguished a neurologist as Charles Mills of Philadelphia said that he had thought of Seguin as ” the best neurological clinician he had ever known,” high praise, as those who had the good fortune to know Charles Mills (60) will realize.
Seguin saw only a limited number of patients each day, so that they might be thoroughly studied; in the evening he elaborated his notes on his day’s work. In 1883 he assembled his various original publications in a single volume, entitled Opera Minora, including one-hundred and eighteen articles on the nervous system, many of them of interest both to the neurologist and the surgeon. His studies on aphasia, published in 1888, were based upon some fifty cases critically evaluated, and this at a time when the problem of cerebral localization was only beginning to be worked out. In a series of lectures to his students at the College of Physicians and Surgeons during the winter of 1877-1878 he covered in a terse and systematic way the anatomical and physiological problems then known. He began his lectures with the spinal cord, then took up the brain stem and cerebellum, and concluded with cerebral localization. more critical appreciation of the clinical significance of the physiology of the central nervous system and its direct application to disease had as yet appeared. Seguin’s clinical approach was threefold, based on the following questions: (a) Is there disease? (b) What is the disease? (c) Where is the disease? These questions being answered the general problem then arose as to the procedure for the cure of the disease or for the relief of the patient.
Following Hammond and Seguin the chair of neurology at Columbia University was occupied successively by Allen Starr and Frederick Tilney. When the Medical School of Cornell University opened its doors in New York, Dr. Charles Dana was immediately selected to fill a similar position there. He had previously held the same appointment at Dart-mouth, whose medical school is one of the oldest in the United States.
In addition to these men, Edward Fisher, Professor of Nervous and Mental Diseases in New York University, Edward Spitzka, at the Post Graduate, and Bernard Sachs, Professor in the New York Polyclinic and Chief of Neurology at Mount Sinai, brought to New York their penetrating insight into the diseases of the nervous system. To these names should be added those of Pearce Bailey, Joseph Collins, Joseph Frankel, Smith Ely Jelliffe, and Abrahamson, all outstanding in a brilliant group.
With the increasing advancement of neurology in New York there became apparent the need, first of a special service, and then of a special hospital, devoted to diseases of the nervous system. Dr. Bernard Sachs (67), following his graduation from Harvard and from the medical school at Strassburg, had the good fortune to be associated with Dr. Gerster, one of the great surgeons of New York, chief of the old German Dispensary and the first chief of surgery at Mount Sinai. Through his enthusiastic support, Sachs, in 1900, secured the assignment of twelve beds, six male and six female, as a neurological service the first such service in this city. Dr. Sachs, who had been consulting neurologist, willingly stepped down to the position of attending neurologist for the sake of one active ward service devoted to neurologic cases. His wisdom and devotion to this service, and to his field, bore fruit in the development of a number of eminent neurologists who received their training at Mt. Sinai.
Some of the earliest work in neurosurgery in New York was directed toward relief of the excruciating pain of trigeminal neuralgia. Indeed, the neurosurgical approach to this disease may be said to have received its great impetus in the United States. The initial attempts for its relief consisted in peripheral section of the trigeminal divisions. This procedure was followed by intracranial section, removal of the gasserian ganglion, subtotal removal of the ganglion, dorsal root section with preservation of the motor root, and finally, differential section.
The earliest operations on the spine were done for fractures and for Pott’s disease (tuberculosis). The first laminectomy of which I have been able to find any record was performed in 1814 by the younger Henry Cline (23) at St. Thomas’ Hospital, London. The eleventh and twelfth spines and one of the arches were removed for fracture of the vertebrae. Cline’s surgical judgment in proposing operation was clearly presented:
In fracture, with displacement of the vertebrae which compresses the spinal cord, this great nervous cord is under precisely the same circumstances as the brain when pressed by the fractured skull, and therefore, as the elevation of the pressing bone is indicated in the latter case, and often effected with success, so is it equally called for in the former, and no positive reason could exist why the operation should not be successful, provided the injury to the spinal cord itself were not a great condition, which, as regards the brain, would equally forbid operation or render its success improbable or impossible.
It was long known that paralysis due to Pott’s disease was usually not the result of direct involvement of the spinal cord but was caused by and was proportionate to the degree of pressure exerted on the cord by the exudate and, in rare instances, by the diseased bone itself.
Percival Pott had noted that ” the useless state of the limbs is by no means a consequence of the altered figure of the spine, or of the disposition of the bones with regard to each other, but merely of the caries” and centuries earlier Hippocrates and observed: “The palsy of the legs and arms, the wasting of the body, and the retention of the urine happen chiefly when there is no spinal deformity… and less frequently in cases of gibbous or angular deformity.”
Abbe (4) 1890; Wyeth (83) 1890; and Gerster (38) all reported relief of symptoms of spinal cord pressure in the presence of Potts disease by laminectomy. Fortunately, this is now a rare affliction and pressure on the cord a still rarer complication. Before Lister’s antiseptic regime, spinal surgery had most often been followed by meningitis and death; hence any operation upon the spine, as upon the brain was regarded as a most hazardous procedure. This view unfortunately tended to persist into the period when the operation could be safely done. It happened, however, that Lister’s earliest contributions were made in Glasgow, where Macewen, a surgeon of great ability, was at hand to seize upon them. This fortunate coincidence accounts in part for Macewen’s early successes. It was also to his advantage to be associated at the infirmary with a distinguished neurologist, Dr. Alexander Robertson, who, as early as 1866, was interested in neurophysiology and localization of cerebral function.
Horsley (40) was the first to remove an intradural spinal cord tumor, on June 9, 1887. His report was read before the Royal Medical and Chirurgical Society of London, a year later, June 12, 1888. The first removal of a tumor of the spinal cord in New York was done by Abbe (1), May 26, 1888, without knowledge of Horsley’s achievement.
Horsley assembled from the literature fifty-eight examples of spinal cord tumor showing that in 74 of the extradural and 83 of the intradural cases the patient died from the indirect effects of the tumor, such as septicemia from bed sores, acute nephritis from urinary retention, and pneumonia. Thus, in some 80 of the cases relief might have been given by surgical intervention. Some of Horsley’s remarks in connection with his own case have an all too familiar sound to the neurosurgeon in search of a spinal cord tumor. He first removed the spines and laminae of the fourth, fifth, and sixth thoracic vertebrae but, on opening the dura, he found no tumor. A lamina above and a lamina below were then removed
What neurosurgeon has not had this experience in spite of every clinical effort to establish an exact level preoperatively!
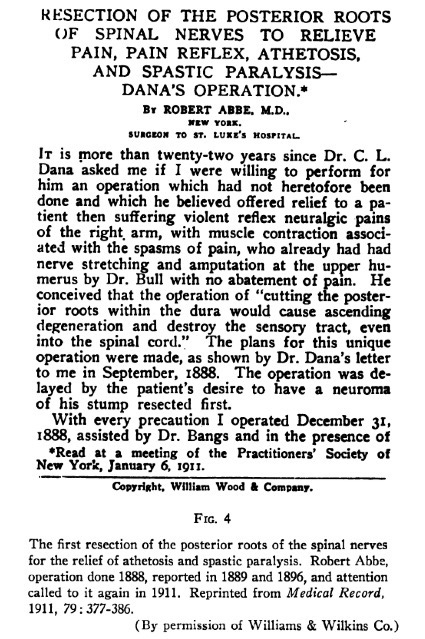
In Abbe’s case the spines and lamina of the eighth, ninth, and tenth thoracic vertebrae were removed, exposing a dense mass of tissue compressing the cord. At the time of his report before the New York Medical Society in February 1889, his patient was able to walk without support, though he had previously been paralyzed, anesthetic, and incontinent of urine. The wound was well healed. The patient remained well for two years; then, some discharge appeared in the wound, and the mass was consequently assumed to have been tubercular.
A second spinal cord tumor was removed by Abbe in April, 1890
This lay extradurally bencath the arches of the eighth, ninth, and tenth vertebrae, extending between the arches and pedicles and into the sub-pleural space. Unfortunately, operation had been postponed so that at the time it was performed the patient was suffering absolute anesthesia below the waist, complete paralysis, incontinence of bowels and bladder, acute nephritis, with 20% albumin in the urine, chills, and fever (102.2°).
Seguin (79) also commented from the neurologist’s point of view. He insisted that a diagnosis of brain tumor should be worked out in not less than five lines of inquiry as follows:
- The diagnosis of a tumor of the cerebrum
- The diagnosis of the exact location of the tumor
- The diagnosis of the depth of the tumor
- The diagnosis of the solitude or multiplicity of the tumor
- The diagnosis of the nature of the tumor
To the discussion of these five ends he brought a keen mind, well versed in neuroanatomy and neurophysiology and skilled in deductive clinical reasoning.
Excerpt from the Bulletin of the History of Medicine Vol. 26, No.4, EARLY NEUROSURGERY IN NEW YORK, Byron Stookey, Distinguished Neurosurgeon
About the Journal Article Writer
Before retiring in 1952, Dr. Stookey was a professor of neurosurgery at the College of Physicians and Surgeons of Columbia University and attending neurosurgeon at the Neurological Institute of the Columbia-Presbyterian Medical Center. An authority on spinal surgery, he was said to be the first in his field to study the rupturing of the intervertebral discs, the pads of muscles between vertebrae. He also made early studies of the treatment on “tic doleureux,” a painful facial spasm. Dr. Stookey remained a consultant to the Presbyterian Hospital and others after retiring and began to study the development of early American medicine. Besides papers and books on neurosurgery, he wrote “A History of Colonial Medical Education in the Provinces of New York, and Its Subsequent Development (1767-1830),” published in 1962. He was born in Belleville, Ill., the son of a physician. He studied at Harvard and in Europe, served in the British Royal Army Medical Corps at the beginning of World War I and then went to the United States Army Medical Corps as a major. Dr. Stookey joined Columbia in 1919. In 1959 the university awarded him an honorary Doctor of Science degree. He was president of the Society of Neurological Surgeons in 1939-1940 and the New York Neurological Society in 1944-1945.
