I shouldn’t be here.
The phrase keeps circling around in her mind, but there she was, she was where she was meant to be. “For every prisoner who had touched my heart and who in turn enhanced my life…”
Continuing from where we have left off, Khan let drop that some prisoners have resorted to catching pigeons through the window, killing them and boiling them in his kettle. That’s no something he’d admittingly do! There is a provisional training for prisoners to help them rehabilitate back to society like cooking classes etc.
Every day, our doctor worked at Huntercombe, she was required to visit the segregation unit or ‘Seg’. It was just a long corridor from healthcare, and consisted of five small cells where prisoners who either need reprimanding or, perhaps, protection and close observation were held. It is a prison requirement at least three a week, the Seg is visited by a doctor to ensure the occupants can cope with the conditions it imposes on them. During the doctor’s time at Huntercombe, the cells in the Seg were often unoccupied. The types of prisoners arriving there were less likely to cause trouble.
If you missed part 1 of the series check it out by clicking here!
Providing health care for prisoners has historically been the responsibility of the prison service, not the NHS. Prison governors have been responsible for allocating resources to health care, but there is considerable variation between prisons in the way in which health care services are provided. Prisons face many problems in the provision of health care, in particular relating to the need for security and inmates’ isolation from their communities.
Describing the prison population
The prison population has three key features: it is largely young, overwhelmingly male and has a very high turnover. About 60% of inmates are under 30 years old. Fewer than one in twenty prisoners are female. New receptions per year amount to four times the prison population. Local prisons, which receive remand prisoners directly from the courts and prisoners on short sentences, have the highest turnover. Training prisons and high security prisons, which hold prisoners on longer sentences have a lower turnover. About one in five prisoners are on remand, that is they are awaiting legal proceedings or sentencing. Prisoners are drawn from lower socio-economic groups and have poor levels of education. Ten per cent of the prison population is black.
Prevalence and incidence of health problems
The range and frequency of physical health problems experienced by prisoners appears to be similar to that of young adults in the community. However, prisoners have a very high incidence of mental health problems, in particular neurotic disorders, compared to the general population. By ICD-10 criteria, in any week, almost half of prisoners are suffering from a neurotic disorder such as anxiety or depression. One in ten prisoners has suffered from a psychotic disorder in the past year. Suicide is about eight times more common among prisoners than in an equivalent community population. Suicides most frequently occur within the first weeks and months of imprisonment. Incidents of deliberate self-harm are reported in one in sixty prisoners a year. Half of prisoners are heavy alcohol users and about one in twenty has a serious alcohol problem. About half of prisoners are dependent on drugs (principally opiates, cannabis and stimulants) and at least one quarter have injected drugs. A minority of prisoners continue to use drugs while in prison.
Services available
Opportunities for informal care and self-care are very limited in prisons. Per capita expenditure on formal health care services are higher than equivalent expenditure for young adults in the NHS. Directly employed health care staff include health care officers (prison officers with some training in nursing), nursing staff (some whom may also be prison officers) and medical officers. Many prisons also contract with local general practitioners, hospital trusts, medical, dental and other specialists. In addition to access to NHS in-patient facilities, many prisons also have their own in-patient facilities. A substantial part of the work of prison health care services involves routine medical examination at entry and prior to release and preparing medical reports for legal reasons. Per year of imprisonment, prison inmates consult primary care doctors three times more frequently and other health care workers about eighty to two hundred times more frequently than young adults in the community. Prison inmates are admitted to NHS hospitals as frequently as young adults in the community, but are also admitted to prison in-patient facilities two to sixteen times more frequently than this. Inmates are also heavy users of medical specialists and professions allied to medicine.
Effectiveness of services
There is little direct evidence of the effectiveness of health services in a prison setting. Relevant data are available from a range of sources of evidence-based reviews and guidelines. It is known that screening prisoners at reception fails to identify many who are mentally ill. There are effective means of managing many of the health problems of prisoners. There are a range of effective treatments for minor illnesses, some of which are available without prescription. There are a range of medications and some psychological treatments (in particular cognitive behaviour therapy) which are effective for neurotic disorders and symptoms. For a range of health problems, the work of doctors can be successfully carried out by other professionals using clinical guidelines.
General features of the health care needs of prisoners
Prisoners have general health needs similar to those found in the general population. These are often overshadowed by health care needs related to offending behaviour such as substance misuse and mental health problems. Prisoners also have health care needs which are a consequence of imprisonment. Imprisonment restricts access to family networks, informal carers and over the counter medication; the prison environment can be overcrowded and may be violent; prisoners suffer emotional deprivation and may become drug abusers or develop mental health problems whilst incarcerated. Other health care needs may be made more complicated by imprisonment such as the management of chronic diseases like diabetes or epilepsy. Finally, certain health care needs are requirements of the prison system itself, for example health screening on arrival at prison and assessments carried out to determine a prisoner’s fitness to appear in court.
Responsibility for the health care of prisoners
The health care of prisoners has historically been funded and organised separately from the National Health Service (NHS) and is the responsibility of HM Prison Service. The broad aim of the prison health care service is: ‘to provide for prisoners, to the extent that constraints imposed by the prison environment and the facts of custody allow, a quality of care commensurate with that provided by the National Health Service for the general community, calling upon specialist services of the NHS as necessary and appropriate.’ (Standing Order 13. Health Care. Home Office. HM Prison Service).
Most health care in prisons is primary care. However healthcare delivery in prisons faces a significant number of challenges not experienced by primary care in the wider community:
The primary purpose of prison is custody and rehabilitation and the need to provide primary health care in such a setting, places constraints and duties on doctors, nurses and other health care staff1.
Models of health care provision in prisons
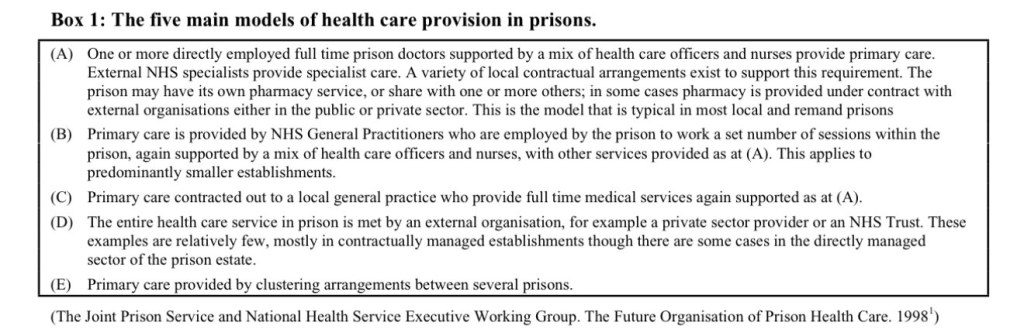
Levels of health care provision
Health care provision is currently organised around prison health care centres. Four categories according to the level of service provided have been identified1:
• Nursing cover during office hours or less.
• Nursing cover from the time of unlocking to lock up.
• Twenty four hour nursing cover with an in-patient unit.
• Twenty four hour nursing cover with an in-patient unit providing services to a number of prisons (cluster centre).
Providing health care in a custodial setting
There are particular challenges in maintaining a healthcare ethos to thrive in an environment where the highest priorities are maintaining order, control and discipline13. These include:
• Custody affects care in that it removes the opportunity for self-care and independent action, inmates have to ask staff for the most simple health care remedies.
• The health care teams’ access to inmates may have to be curtailed in the interests of security.
• The proposed actions of medical staff may clash with security considerations.
• Nurses may be asked to carry out duties unrelated to health care.
• Some patients may be manipulative, try to obtain medication they do not require and create suspicion amongst health care staff of all prisoners.
• The health care centre is often seen as a sanctuary or “social care” option for some prisoners, in particular those who are being bullied.
Describing the prison population
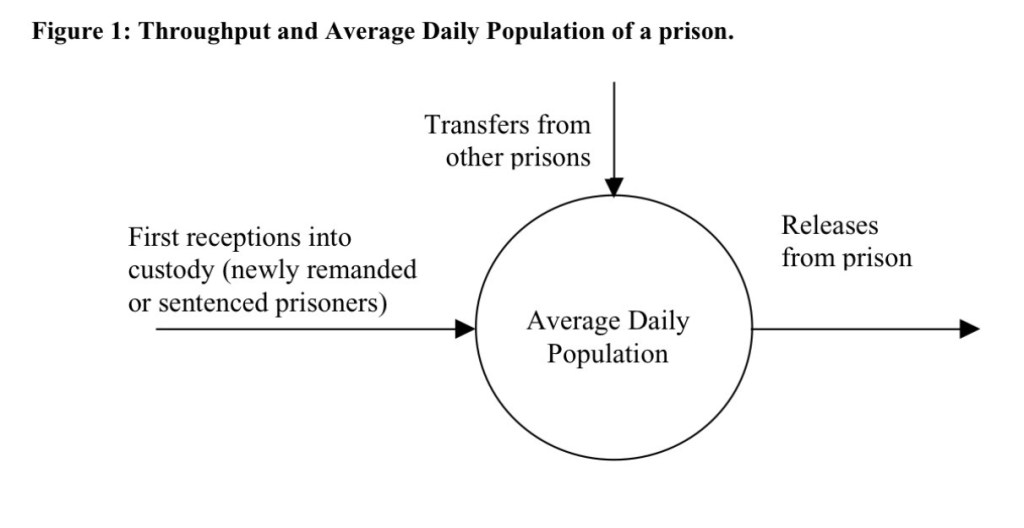
The prison population can be described numerically in a number of ways. The first of these is the Average Daily Population (ADP). This refers to the average number of prisoners in the prison at any one time. The second, New Receptions, refers to the number of new prisoners arriving in the prison in a given time period. In any one prison, the total number of new receptions is made up of newly sentenced or remanded prisoners (referred to as New New Receptions) and prisoners who have been transferred from other prisons.
Sub-categories of health care needs
Sub-categories of health care needs are used to enable planners of health care services to recognise and manage the different requirements for services that sub-groups in a single population or disease group may present. There are a number of ways in which the health care needs of the prison population could be sub-categorised.
Categorisation by type of prison
The health care needs of establishments depend to some extent on their primary function, as this will affect the type and turnover of inmates and their general health problems. One method of sub-categorisation would be to categorise by the type of prison, i.e.
• Prisoners in Young Offender Institutes
• Prisoners in Women’s Prison
• Prisoners in Training establishments/Open prisons
• Prisoners in Local Prisons/Remand centres
• Prisoners in High Security Prisons
Categorisation by type of health problem
Health care needs of prisoners could also usefully be sub-categorised by diseases and health problems. This is because many of the health problems found in a prison setting are common in all types of establishment regardless of age or sex. There are health problems that:
Are important in primary care outside of prisons:
• These include the commonest reasons for consultation in the (non-elderly) general population, for example, epilepsy, asthma, diabetes, infectious diseases, dental health, minor and self-limiting diseases and neurotic disorders.
Are risk factors for (or associated with) criminal behaviour:
• These health problems include mental disorders which appear to dominate the workload of the Prison Health Care service despite official policy encouraging early diversion of mentally disordered offenders from custody to hospital, i.e., personality disorders; functional psychoses; and substance misuse.
Are associated with imprisonment:
• These are health problems that may arise because of imprisonment and include neurotic disorders, self-harm and suicide.
Are a consequence of, or are associated with poverty:
• As described in the previous section the unemployed, and homeless are over-represented in the prison population. Therefore health problems that are more prevalent in these groups will be more prevalent in the prison population than in the community. These include epilepsy, asthma, Ishaemic heart disease, dental health problems and infectious diseases.
Are particularly difficult to handle in the prison environment:
• This particularly refers to maternity care.
Other sub-categories
The health care needs of prisoners could also be sub-categorised by length of stay (short, medium or long stay), category of prisoner (remand or sentenced) or the prisoners’ external stability and support (i.e., access to family networks, social services, support groups etc.).
Sub-categorisation chosen for health care needs assessment of a prison population
In the sub-categories described above, a number of health problems could fit into more than one sub-category and would therefore make the process of data collection unnecessarily complicated. As a result of this the sub-categories that will be used through this report are based on type of health problem, and where necessary, within these categories, the type of prisoner.
Main sub-categories
• Minor and self-limiting illnesses
• Physical health problems
• Pregnancy and maternal health
• Mental disorders
• Substance misuse
• Health promotion
Secondary sub-categories
• Age
• Sex
• Remand or sentenced
Health promotion
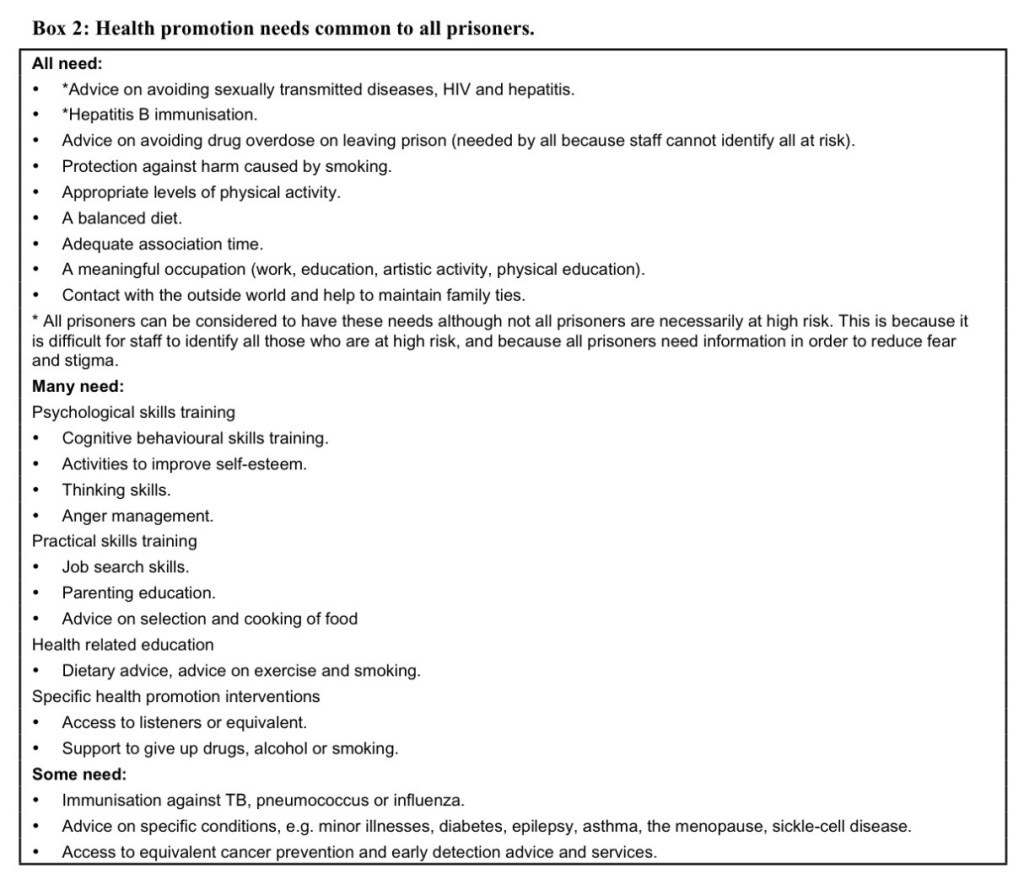
Health promotion needs of prisoners
It may be helpful to consider the health promotion needs of prisoners under three headings. Needs that all prisoners are likely to have, needs that many prisoners are likely to have and needs that some prisoners have. Examples each of these are illustrated in Box 2.
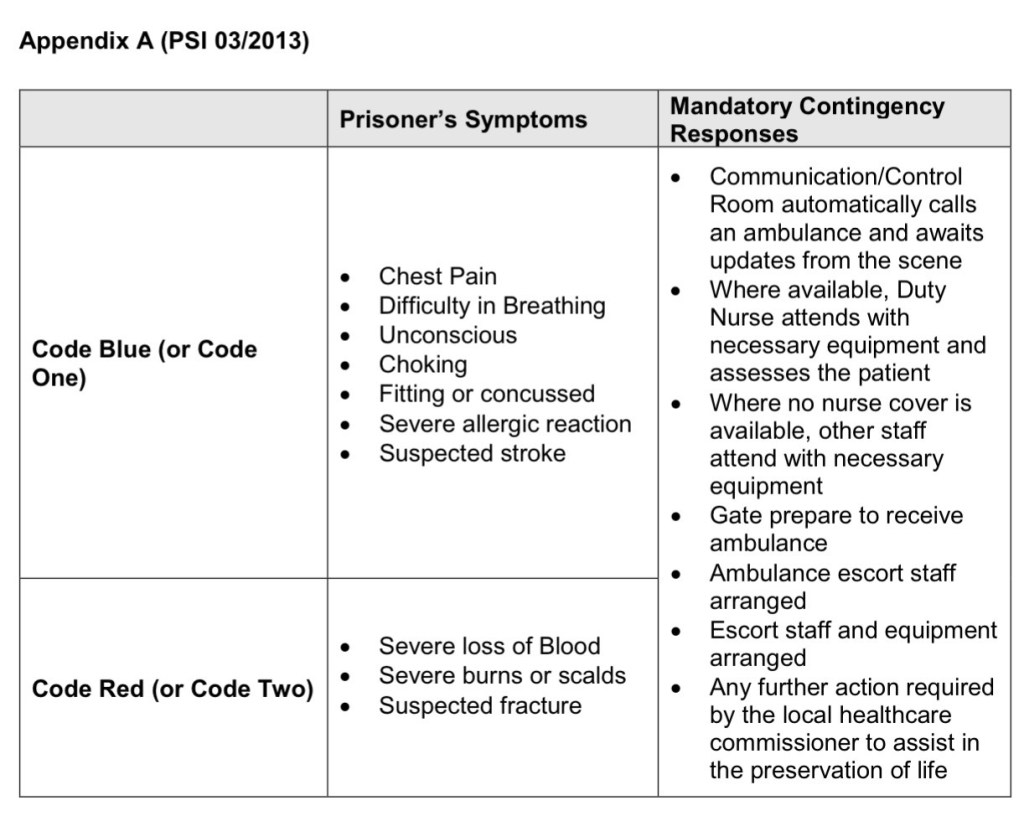
Managing potential medical emergencies
PSI 03/2013, Medical Emergency Response Codes, provides a framework for managing potential medical emergencies. Officers may request the emergency nurse to attend a ‘Code Blue’ (or Code One) or ‘Code Red’ (or Code Two). See Appendix A of PSI 03/2013 (below) for specific clinical presentations and their codes, however simply described, blue means not breathing and red means bleeding.
When faced with a potential medical emergency, baseline observations should be undertaken by the assessing nurse prior to the GP/ANP assessment of the patient. An Early Warning Score assessment should be completed and if there is uncertainty but the patient is not so acutely unwell as to require emergency referral, consider monitoring the Early Warning Score over a documented time interval e.g. hourly observations for the next six hours. This will require collaborative effort, particularly if the prison is in patrol or night state and an officer is required to open the patient’s door to facilitate observations or the EWS deteriorates and an emergency escort to hospital is required.
Make clear appropriately detailed notes on SystmOne
Make clear appropriately detailed notes on SystmOne for every patient encounter, whether face to face, providing advice to other colleagues in the healthcare team or prescribing. It is very likely that, at some point in your career in prison healthcare, you will be asked to attend a Coroner’s Court since all deaths in custody are subject to external scrutiny, whatever the circumstances of death as the deceased was under the care of the state. You may also be required to write a witness statement for legal challenges made to the care given by the healthcare team. This may be several years or more since you saw the patient and therefore, your notes are likely to be the only source from which to respond and will be your evidence.
In addition to clear documentation on SystmOne, it is important to share appropriate information with prison colleagues in order to manage risk. This information may be used to inform the ACCT process of self-harm and suicide prevention or to share intelligence that is relevant to the safety of the patient or to others around them in the prison. There will be an observation book on each wing in which prison staff record pertinent entries and in addition information is recorded on the NOMIS system.
If you are a prescriber, check if there is a prison formulary, treat in line with local and national policies and remember you are part of a multi-disciplinary team
When you start out working in a secure environment, you may be singled out by prison residents as being a potential ‘soft target’ for prescribing drugs that may be diverted, traded or abused. As well as more obvious dependence forming medicines, you may be asked to prescribe drugs that would not normally be associated with misuse in the community e.g. T-gel, E45, Aveeno, inhalers, deep heat, pseudoephedrine, loperamide, Gaviscon, ranitidine, cimetidine, cyclizine, mebeverine, hyoscine butylbromide (Buscopan), lactulose, Rectogesic, Anusol, insulin, orlistat, food supplements, TENS machines, paraffin-based products.
***
THE EVENTS TAKE PLACE AROUND FEBRUARY 2014 TO APRIL 2014
Habib Khan
She shared a comfortable ten minutes of her conversation with Habib Khan.
Kofi Aboah
She increased the dose of his painkillers and he went to the oncology clinic for blood tests. Under the Facilitated Returns Schemes, he agrees not to return to the UK within a period of five years. And in a month’s time he will be receiving a final payout of £250. He spoke to his wife through the embassy on video call.
Usama
Suddenly, code blue was called over the officers’ radio and the doors to the Seg crashed open. ‘Should I have seen something else? Should I have realised that this was a man who was close to the edge?’ They were all looking out for him as a collective team, this included the officers, he was on the ACCT book more often than he was off. Prisoners identified as being at risk of suicide or self-harm are put under the Assessment, Care in Custody and Teamwork process to keep a close watch on them. In perspective it was easy to blame oneself in hindsight. An officer found him, thought he was a dead man, there was a torn strip of his sheet round his neck, and the other end was tied to the radiator. The officer untied the knot with the use of a fish knife, his voice trailed off, explaining himself to our doctor. Pastor Clive (they have a religious leader of every faith in the prison) started CPR helping the officer keep him alive until the nurses arrived. It is customary that anyone involved in the incident should attend a debriefing with the governor, but our doctor was in no mood to do so. She needed to be alone to process her thoughts and find the strength to get back to work. Saroj, Rosemary and an officer continued to perform CPR. The defibrillator pads were in place and Usama was still alive! She had to be in the last cell on the left of the Howard Wing.
Offender Health should be on the med school curriculum. Do you agree?
https://www.bmj.com/content/384/bmj.q213/rapid-responses
Sources;
The Prison Doctor: THE FINAL SENTENCE
