Evolutionary and Ecological Perspectives on a Cholera Epidemic
Medical anthropology theory is a blend of social science, epidemiological, and biological perspectives on disease. The most effective way to show how these theoretical threads come together in medical anthropology is to introduce them separately.
Theories operate at an abstract level. They reduce the complexity of a given phenomenon to those characteristics that are considered relevant to understanding the pattern under study. This last point about theory is especially important because it helps us to understand the conflicts that arise over competing theoretical interpretations. Often, theoretical disagreements emerge from differences in what scholars think is relevant to an explanation of a phenomenon and what they accept as evidence. No theory can account for all aspects of a phenomenon; all theories are vulnerable to the claim that some relevant factor(s) was not included or that evidence was missing or misconstrued.
Thinking about Epidemics
January is midsummer in Peru. Temperatures soar, and residents of the largest coastal cities migrate to beach communities, either on day trips or for extended vacations. Huanchaco, the fishing village in which I lived during my fieldwork, is transformed on weekends to a virtual Coney Island, as throngs arrive from Trujillo in overloaded buses and packed family cars. Overnight, small kiosks and seasonal restaurants spring up all along the beach; they offer every manner of refreshment, but ceviche, a raw seafood dish, features prominently on most menus. The crowds push the infrastructure of the village, including water supplies and sanitation, well beyond its capacity.
At the end of January in 1991, several years after my research on Peruvian curers had ended, there were reports of an increase in diarrheal illness in Candelaria, another coastal village just north of Peru’s capital, Lima. Laboratory tests revealed the presence of the cholera bacterium. This was the twentieth century’s first appearance in South America of one of history’s most deadly epidemic agents. Within two weeks, 12,000 cases were recorded along the full 2,000 km of Peru’s coast. The epidemic moved rapidly into the Peruvian highlands and then crossed national borders to affect Ecuador, Colombia, and Brazil. It continued to spread throughout Latin America in the following two years, making almost one million people sick and killing nearly 9,000 (Guthmann 1995). Researchers speculate that cholera may now be a permanent part of Latin America’s epidemiological profile.
Epidemics offer particularly vivid demonstrations of the interconnections between biological, social, and cultural components in the human experience of disease. For many of the historically significant epidemics (e.g., of smallpox, the bubonic plague, leprosy, tuberculosis, cholera), there is substantial scientific knowledge about the organisms responsible for the diseases, about the means of transmission, and about treatment and prevention. The links between epidemics and social factors such as urbanisation, poverty, and migration are usually well known today. Finally, because epidemics can be so devastating to human communities, they provide ample opportunity for cultural interpretations as afflicted populations struggle to make sense of their suffering.
History and Biology of Cholera
Historical reports of epidemics likely to have been cholera date back as far as 1503. However, it was not until the early 1800s, during the first pandemic (prevalent throughout a country, region, or the whole world) of the disease (1817-1823),2 that cholera spread from its home in India to Southeast Asia, the South Pacific, China, and Egypt. After a very short pause, a second pandemic (1826-1851) brought the disease to eastern and western Europe (1830), North America (1832), and Latin America (1833) (Kiple 1993). Within three decades, cholera became a global concern.
It was during the third cholera pandemic (1852-1859) that a breakthrough was accomplished in the scientific understanding of how the disease spreads. A London physician, John Snow, noted that the cholera cases that began to appear on August 31, 1853, in the Soho district were concentrated near a public water source on Broad Street. Closer investigation showed that, in addition to those patients who lived near the well, seven male victims who lived elsewhere had consumed its water while working in the neighbourhood. By contrast, the employees of a nearby brewery, none of whom got sick, drank either free beer or brewery water while at work. Snow concluded that the Broad Street well was contaminated and, on September 7, had the pump handle removed. The outbreak subsided almost immediately. It was later discovered that a leaking cesspool had introduced cholera bacteria into the well, probably on August 28 when a baby had come down with the disease in the vicinity (Diamond 1992).
Knowing that cholera could be spread by fecal contamination of water contributed greatly to public health campaigns, but scientists still had not identified the pathogen (disease-causing agent). It was not until the fifth pandemic (1881-1896) that the German microbiologist Robert Koch and colleagues isolated the comma-shaped bacterium that causes cholera. Seventy-six more years, and one more pandemic (1899-1923), passed before investigators learned how the bacterium triggers cholera’s characteristic, and sometimes fatal, diarrhoea. In 1959, Calcutta researcher S N De identified the toxin produced by the bacterium that causes the small intestine to secrete large quantities of fluids. The precise molecular-level analysis of how the toxin causes potentially fatal dehydration dates to the 1970s (Rabbani 1986).
During the first six cholera pandemics, mortality rates were extremely high: 50-70 percent of those afflicted died. Significant improvements in survival came after the development of an effective rehydration solution (1959—1961),3 an orally administered fluid that replaces the water, sugar, and salts lost through diarrhoea. This inexpensive treatment, commonly called oral rehydration therapy (ORT), contributed to a much lower loss of life during the seventh pandemic, which began in Indonesia in 1961. The 1991 Peruvian outbreak, considered to be the “third phase” of the seventh pandemic,4 had regional case fatality rates as low as 0.69 percent, largely because of the availability of ORT(Guthmann 1995).
At about the same time that the epidemic began in Peru, there were cases reported from south Asia of a new variant, or serotype, of cholera, Vibrio cholerae 0139. Epidemiologists judge this to be the start of the eighth pandemic, the first time in history that two cholera pandemics have overlapped. This development is especially troubling because the old strain appears to offer little or no protection against infection by the new serotype. It is clear that cholera is far from being eliminated from the inventory of diseases that affect humans, even if the loss of life associated with it has been minimised as a result of ORT.
Shellfish taken from such waters, which form an environmental reservoir for the bacteria, may infect humans, especially if the fish is eaten raw or undercooked (Popovic et al. 1993).
Under circumstances of poor sanitation and untreated water supplies, cholera can move through a human population with impressive efficiency. During the first three days of the disease, when diarrhoeal flow is the greatest, the amount of bacteria released daily into the environment from a single sufferer is sufficient to infect up to ten million people (Popovic et al. 1993). However, the disease is not spread by person-to-person contact because exposure to literally billions of bacteria is required for infection to occur.
Epidemiological Accounts of Peru’s Cholera Epidemic
The 1991 cholera outbreak in Peru received a great deal of attention from epidemiologists, who examine “the distribution of disease in large populations to isolate the risk factors that enable intervention and, ultimately, control” (Agar 1996:391). Like medical anthropologists, epidemiologists consider the “biological, social, and cultural causes and ramifications of sickness” (Trostle and Sommerfeld 1996:254). However, epidemiologists are ultimately interested in social and cultural detail only as steps toward a universal explanation for what leads to a specific health problem. For most medical anthropologists, understanding the local context in which health problems arise is itself the goal of research (Hahn1 995:102-103).5
Epidemiological accounts of the Peruvian cholera epidemic focused on the source of the cholera bacteria and how it was transmitted. The fact that the first cases were reported from coastal communities led researchers to speculate on the possibiIity that contaminated seafood, especially shellfish, was responsible for the start of the epidemic. Ceviche, the uncooked seafood dish so popular in Peru, was implicated. The ocean dumping of untreated sewage from coastal cities and/or the release of contaminated ballast from ships were considered likely sources of contamination; a potential contributing factor was the summer warming of ocean currents (Crowcroft 1994).
Epidemiologists unanimously argued that, once the outbreak began, contaminated water supplies had spread the bacteria through coastal populations. Peru’s inadequate and seriously deteriorated municipal water and sewage systems, always strained to the breaking point during the hot summer months when water supplies dry up, were a major culprit. For example, a 1991 study of the water system in Trujillo (Swerdlow et al. 1992), which has a population of more than 300,000, showed no routine chlorination, many illegal connections to pipes with the potential of introducing contaminants, and crops irrigated with sewage water. In addition, water was available in much of the city for only one or two hours a day, which encouraged household storage in tanks that promote bacterial growth. Not surprisingly, cholera was found in 60 percent of samples taken from different locations in the water distribution system.
After identifying the source(s) of the epidemic and the means by which it was transmitted, epidemiological accounts analysed how many people got sick (morbidity) and how many died (mortality). They also reported how many new cases were registered each month and year (incidence) to gauge the course of the epidemic. Calculations of the proportion of the country’s population that was infected at one time (prevalence) indicated how much of a burden the epidemic was to medical and social services.
Comparisons of these standard epidemiological measures between different regions of the country (e.g., coast, highland, and tropical forest) suggested urban/rural differences in the risk of exposure, as well as in access to effective medical care. For example, although the incidence, or “attack rate,” was much lower inland than along the coast, the case fatality ratio was as much as twelve times higher (WHO 1991). In other words, if you lived in a mountain community you were less likely to get sick but more likely to die if you did, because medical services were not as available as in coastal cities.
At the national level, epidemiological statistics described a severe cholera epidemic with very low fatality due to the widespread use of intravenous and oral rehydration. In 1990, Peru’s Health Minister ordered the distribution of 1.3 million ORT kits in anticipation of what he expected would be a bad summer season of diarrhoeal disease (Gall 1993). Once the epidemic began, international health organisations flew in additional supplies of the kits as well as quantities of intravenous rehydration solutions. Urgent public health warnings on television and radio were also credited with keeping mortality low in coastal cities.
Cholera and the Evolutionary Framework
How are evolutionary theory and the ecological model applied to the analysis of cholera? In a Discover magazine article, UCLA professor of physiology Jared Diamond gives an account of the Peruvian epidemic that draws on evolutionary theory to explain the interaction between cholera bacteria and human hosts (Diamond 1992). He asks that we think about this interaction from the bacteria’s point of view: How does an organism (the bacterium) that cannot move on its own manage to get itself spread to the greatest number of additional hosts in which it can reproduce? Diamond points to the selective advantage represented by the cholera bacteria’s production of a toxin that disturbs the normal reabsorption of liquid from the small intestine back into the blood system: This produces a severe diarrhoea that sends the microbes out to infect new hosts.
Casting cholera’s activity in terms of a combat metaphor (see Chapter 1), Diamond notes that there is some variation in the way different strains of the bacteria accomplish this reproductive feat: “Some microbes aim for total victory, in the form of massive diarrhoea that kills the patient after broadcasting billions of microbes within a few days. Others settle for a truce, whereby the host survives with chronic low-level diarrhoea that sends out a small, steady stream of microbes” (p. 64).
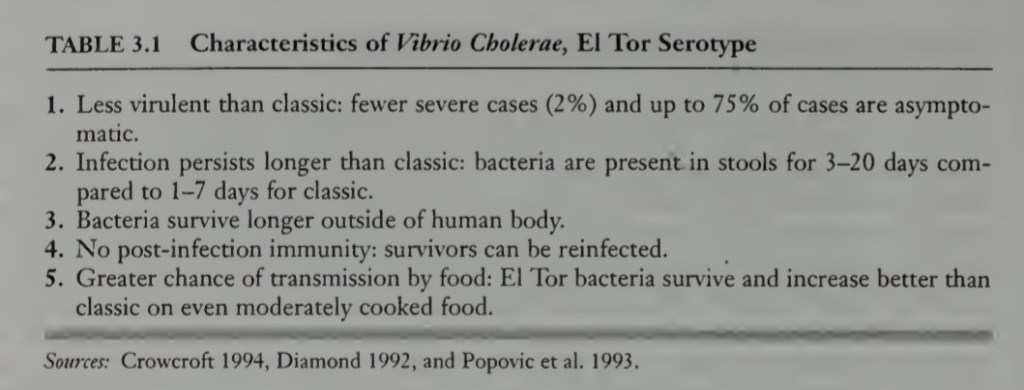
The conditions of each new cholera outbreak, including the preventive and treatment measures available to human communities, will benefit one or the other “strategy.” Wemight ask, for example, what conditions contributed to the dominance in recent outbreaks of the El Tor variant of the cholera bacterium. Consider the twentieth century’s development of public health infrastructures and epidemic control measures in the light of the following comparisons between El Tor and Classic variants of cholera:
• El Tor is less virulent than Classic. El Tor infection lasts longer, but there are fewer severe cases; as many as one-fourth of those affected have only moderate diarrhoea and there is a higher rate of asymptomatic carriers (i.e., the bacteria cause no discernible symptoms).
• El Tor bacteria are excreted in stools for between three and twenty days, compared with one to seven days for the Classic variant. Once shed, El Tor bacteria survive longer outside the human body. They have been shown to grow to higher numbers on moderately cooked food than Classic bacteria (Popovic et al. 1993).
• Exposure to El Tor bacteria produces virtually no post infection immunity, compared with a temporary immunity after exposure to the Classic type.
We are not in a position to identify with any certainty the conditions that gave El Tor a measure of evolutionary advantage over Classic variants in recent outbreaks. However, several changed circumstances in the twentieth century are likely to have been involved. First, the worldwide movement of human beings via systems of mass transportation certainly made the communication of cholera from one region to another far easier. Second, the increasing concentration of human populations in urban centers, especially in the Third World, has far outpaced the ability of public services to accommodate the increased numbers. For example, Lima’s population rose from 645,000 in 1940 to 6.5 million in 1990 (Winn 1992:246). As a result, water and sewage systems, as well as state-sponsored regulation of hygiene in food production and sales, have been seriously compromised in countries around the world. A third factor identified by some analysts is human-induced global warming, which may contribute to larger ocean blooms of plankton on which cholera bacteria survive to be transmitted to shellfish and then to humans (Epstein 1992; Guerrant 1994).
Unfortunately, there is another alternative: Infect so efficiently and severely as to overwhelm any epidemic control measures. Cause the maximum diarrhoea in the shortest time possible and to the largest number of humans available—even if the hosts die as a result. And, ideally, select a country that is ill prepared, logistically and/or politically, to respond to a public health emergency. The 1991 appearance in Southeast Asia of the new serotype Vibrio cholerae 0139, with reported case fatalities of 5 percent and with faster transmission than El Tor (Crowcroft 1994), may represent a selection for a more virulent strain. Longer experience with tins variant is needed before we can speculate on its survival advantage.
The ecological/evolutionary analysis of cholera highlights the impact of changing human demographic, economic, and medical patterns on the bacteria’s evolutionary trajectory. The combination of evolutionary theory with the ecological model has also provided insights into the long-term genetic implications for human hosts of exposure to other epidemic agents. An excellent example is the interdisciplinary investigation of kuru, a central nervous system disease found among the Fore people of New Guinea (see Lindenbaum 1979).
This shortcoming notwithstanding, the ecological/evolutionary model found an early and welcome reception in medical anthropology. It fit well with a resurgence of anthropological interest in the relationship between human societies and the environmental constraints with which they contend.9 It also resonated with a renewed interest in the applicability of evolutionary theory to anthropological evidence.10 For a discipline in search of a theoretical framework that transcends the particularistic studies of individual cultures, the model had great appeal.
Medical Anthropology Embraces the Ecological/Evolutionary Model
The introduction of the ecological/evolutionary model of disease into medical anthropology is traceable to an influential early textbook written by Columbia University anthropologist, Alexander Alland (1970). Alland had earlier championed an extension of the evolutionary concept of adaptation to include not just the long-term results of natural selection on gene pools, but also the far more rapid processes of “cultural evolution” (Alland 1966, 1977). He argued that the uniqueness of humans is that they adapt, or fail to adapt, to the survival challenges of their environments through genetic, developmental (i.e., physiological changes during the lifespan), and cultural means.
This last use of the notion of adaptation is significant because it broadens the concept to include both somatic (bodily, physical) and extrasomatic (behavioral) human characteristics. A good example of the contrast is the physical (somatic) response to extreme cold—constriction of blood vessels and shivering—versus the fabrication of clothing and shelters that protect from the cold (extrasomatic) (see Frisancho 1981:41-84). Here is how Alland explains why he uses the adaptation concept for both kinds of responses:
It is often pointed out that the major difficulty in applying Darwinian evolution to so-called cultural adaptation is the fact that culture traits are extrasomatic and therefore not bound to genetic mechanisms. Hence it is said, quite correctly, that different rules govern their transmission. They are not only passed from generation to generation through a learning process, but may easily transgress societal boundaries without concomitant interbreeding. But how important is this difference? As I have pointed out above, adaptation is the major concern here, not the origin of traits nor the mechanisms of their transmission. The relationships between traits and environments have the same effect on adaptation whether the traits are biological or cultural, and adaptation in human groups is bound to be the result of combined biological and cultural forces. (Alland, in Landy 1977:42)
Alland noted that applying the concept in medical anthropology offers the advantage of quantifying how successful or unsuccessful a social system is in meeting the goals of survival and reproduction: Rates of morbidity/mortality and fertility/fecundity are direct measures of how well a social system has adapted to its environment.14 Thus, Alland would cite the low mortality rates in Peru’s cholera epidemic as evidence of that country’s successful (cultural) adaptation to the disease.
Alland’s use of the adaptation concept and the evolutionary/ecological model is not unique to him or to medical anthropology. Anthropologists studying human population biology have elaborated increasingly complex models of human adaptation. Like Alland, they use the term adaptation to refer to the entire range of adjustments genetic, developmental/physiological, and cultural—that aid in biological function (Baker and Weiner 1966; Frisancho 1981; Ulijaszek and Huss-Ashmore 1997).1
The adaptation concept has also been central to the field of cultural ecology, which analyzes socioeconomic arrangements in terms of the payoff they offer for human physical well-being.16 Alark Cohen’s Health and the Rise of Civilization (1989) is an ambitious and often-cited survey of the conclusions of this research. He summarises the health risks and benefits of general types of human societies: hunting and gathering bands, sedentary agricultural communities, and large states. Among the health factors that Cohen considers are nutrition, exposure to infectious disease, and fertility and mortality patterns. Particularly intriguing, given stereotypes of the barely surviving hunting and gathering band, is Cohen’s conclusion that many of the infectious diseases that plague settled human communities are insignificant in small-scale nomadic societies.
Within medical anthropology, Alland’s model has been elaborated by Ann McElroy and Patricia K Townsend in their teaching text Medical Anthropology in Ecological Perspective (1996). McElroy and Townsend adopt the term medical ecology, which they define as “the study of health and disease in environmental context” (p. 5). Their approach is drawn directly from the synthesis of ecological and evolutionary models urged by Alland. Following Alland, they use the concept of adaptation in all three senses: genetic, physiological, and cultural.
McElroy and Townsend’s work has generated a strong line of criticism from critical medical anthropologists. The ensuing debate deserves our attention. In the next chapter, I introduce the critical and interpretive perspectives and illustrate both with further explorations into the cholera epidemic.
Sources;
Paragraph Bits Extracted from Exploring Medical Anthropology, Donald Joralemon
