Some treat their curing work as a divine calling; others seem more like pragmatic businessmen. Yet, there are striking similarities in the paths that led these exceptional individuals to the occupation of curandero, and there is an underlying curing philosophy that unites them. Our primary objective is ethnographic, to record in detail the symbolic system which is the foundation of Peruvian north-coastal shamanism. However, the alternative of burying mesa inventories and ritual descriptions in a series of appendices would imply that these are somehow peripheral to the story of curanderismo. Our informants consider it otherwise. It is important to keep in mind that Peruvian curanderismo is a grassroots healing tradition that has at various times been subject to official condemnation and repression. This has inhabited the formulation of the kind of explicit theoretical basis that constitutes the shared therapeutic framework of other ethnomedical systems. Peruvian curanderos see their work in individualistic terms and would find questions posed at a general level impossible to answer. They will tell you what they personally think and do, but they leave it to the researcher to piece together from their idiosyncratic accounts the components of the curing philosophy they share. This is the difficult task that Sharon undertook when he began interviewing his first curandero informant, Eduardo Calderón, and which we take a step further with the additional ethnographic information presented here.
Eduardo Calderón
I have written at length about Eduardo Calderón, including how I came to know him in 1965 (see Sharon 1978:1-22), and so will only briefly summarize here the details of his life. However, for those unfamiliar with Eduardo from my publications and/or the ethnographic film, Eduardo, the Healer (Cowan and Sharon 1978), I will begin with a few general characterizations.
Possessed of a warm, extroverted personality and a robust sense of humor, Eduardo Calderón immediately impressed me when we first met in July 1965 at the archacological site of Chan Chan outside of Trujillo where he was the artist in charge of adobe frieze restoration. A formidable raconteur, he seemed capable of an infinite variety of facial expressions as he recounted story after story based on his unusually rich life experiences. Fisherman, artist, teacher, curandero, he had learned much about human nature, its strengths and frailties, and had emerged a confident and able spokesperson for the merits of traditional forms of healing. My apprenticeship with him over the course of seven years’ was both an intellectual adventure and a close friendship.
Biography
Eduardo (“Chino”) Calderón Palomino was born in 1930 in Trujillo, where his parents lived after migrating from the sierra near Cajabamba. Having to work from an early age, and being an adventuresome child, Eduardo made slow progress in school, finishing only first grade by the age of ten. His preference for wandering about the countryside eventually earned him the nickname “Tuno” (truant, cunning rogue), but it also led him to explore many of the archacological ruins that surround Trujillo. He collected potsherds and artifacts, and he developed a lifelong interest in the art of pre-Hispanic cultures.
The cause of Eduardo’s restlessness during those years, however, went deeper than mere childhood mischief. He remembers disturbing dreams and visions that he had during his early childhood and recalls fearing the ridicule of others if he were to share with them his experiences. As a result, he turned inward, keeping the frightening images to himself. It was only in later adolescence, when he began to develop a real intellectual curiosity, that he found some relief from his psychic tensions by dedicating himself to his studies.
Feeling a “calling to serve humanity,” Eduardo enrolled in Trujillo’s seminary instead of in the public high school, but he rebelled against the discipline of orthodox religion and left the seminary in his final year. Financial constraints prohibited Eduardo from pursuing his next preference, a career in medicine; however, a longtime interest in art, with skills learned from his artisan father, provided a good outlet for his creative spirit. Eduardo showed a special talent for sculpture in clay, wood, and stone. After captaining his weightlifting team in the national championship competition in Lima, he remained in the capital and enrolled in the School of Fine Arts. He worked with his uncle as a bricklayer to pay for his night-school classes.
Life in Lima was traumatic for Eduardo, both personally and professionally. An academic approach to art conflicted with his less-disciplined, freedom-loving spirit, and he left art school before completing his first year. A marriage to a classmate was broken up by meddling in-laws, who disparaged Eduardo’s humble origins and sent their daughter to live with relatives. After failing to locate his spouse, Eduardo returned to Trujillo in late 1951, took up life as a fisherman in a small seaside hamlet nearby, and occasionally exhibited his art in the city. In the meantime his wife gave birth to a child of his that Eduardo has never seen.
At the end of the period he spent in Lima Eduardo had suffered from a mysterious ailment that failed to yield to modern medical treatment. Since both of his grandfathers had been curanderos in the highlands, it was natural that Eduardo’s family would decide to consult with a folk healer. Eduardo was treated and cured by a female curer, or curandera. Like the classic “sickness vocation” discussed by Eliade (1964:33-36), this experience inspired Eduardo to explore the world of curanderismo. He attended a few ritual sessions and then accompanied a friend suffering from the effects of a love spell to Chiclayo where they both participated in a séance conducted by an enguayanchero, or maker of love spells. Not only was his friend cured, but Eduardo experienced “visión” (psychic in-sight), which helped in the cure. Eduardo declined the sorcerer’s offer of an apprenticeship, however, knowing intuitively that he was not inclined toward this darker side of curanderismo.
Once back in Trujillo, Eduardo began to learn more about curanderismo from the uncle of his second wife, Maria. He initially went to this relative in order to remove a spell intended to “pull” him into the service of the Chiclayo sorcerer. Gradually, however, while working as a stevedore on the docks of Trujillos port (Salaverry), fishing in Chimbote, and exhibiting his art in Trujillo, Eduardo also became the uncle’s main assistant, or rastreror (“tracker,” one who helps the curandero “see” during curing ses-sions). His powers developed and, in one critical ritual, he felt called by the “Christ of the mesa” to effect part of the session. However, since he still did not feel competent enough to set up his own mesa, he pursued further apprenticeships with curanderos in Chiclayo, Mocupe, and Ferreñafe, where he learned the extensive lore relating to “power spots” invoked by curers (e.g., the mountains of Chaparrf and Yanahuanca and the sacred lagoons of Las Huaringas).
After four years of training, at the age of twenty-eight, Eduardo performed his first cure, for a cousin. Thus he began his career as a curandero, working with his own mesa and vowing to God never to abuse his powers and to work for good in the service of humanity.
Eduardo’s growth as a curandero paralleled his development as an artist. In the early 1960s, after several years as a practicing curer, he had the opportunity to produce a great deal of wood sculpture for the appreciative staff of the American hospital ship Hope. His enhanced reputation as a local artist led him to be hired in the mid-1960s to direct restoration work at the archaeological site of Chan Chan, near Trujillo. During this time he also taught ceramics and was involved in the production of replicas of pre-Columbian ceramics for sale to tourists.
When the Chan Chan project ended in the carly 1970s, Eduardo set up his own ceramic workshop and divided his time between ceramic production, teaching, and attending to the needs of the large number of patients who sought his services as a curandero. By the mid-1970s he had quit teaching and had set up a restaurant adjacent to his workshop. In the late 1980s he built a hostel near the expanded restaurant and contracted for the construction of three motorized launches to be used in a projected fishing business with his sons.
Through his exposure to archaeology and pre-Columbian ceramic motifs Eduardo learned much about the pre-Hispanic past of the north coast. Thus, in a very real sense, Eduardo’s artistry has led him to a rediscovery of his cultural heritage. This has also been true of his shamanism. Together, art and shamanism have complemented his personal search for meaning.
He does not believe in keeping his knowledge a secret and freely shares his ideas with any sincere person who inquires about curanderismo:
“It is necessary to teach all so that they know what it is all about. One must never keep secrets-secrets that are not secrets. Rather, one must bring all out into the light (Calderón, in Sharon 1978:xiv).”
Calderón’s Mesa
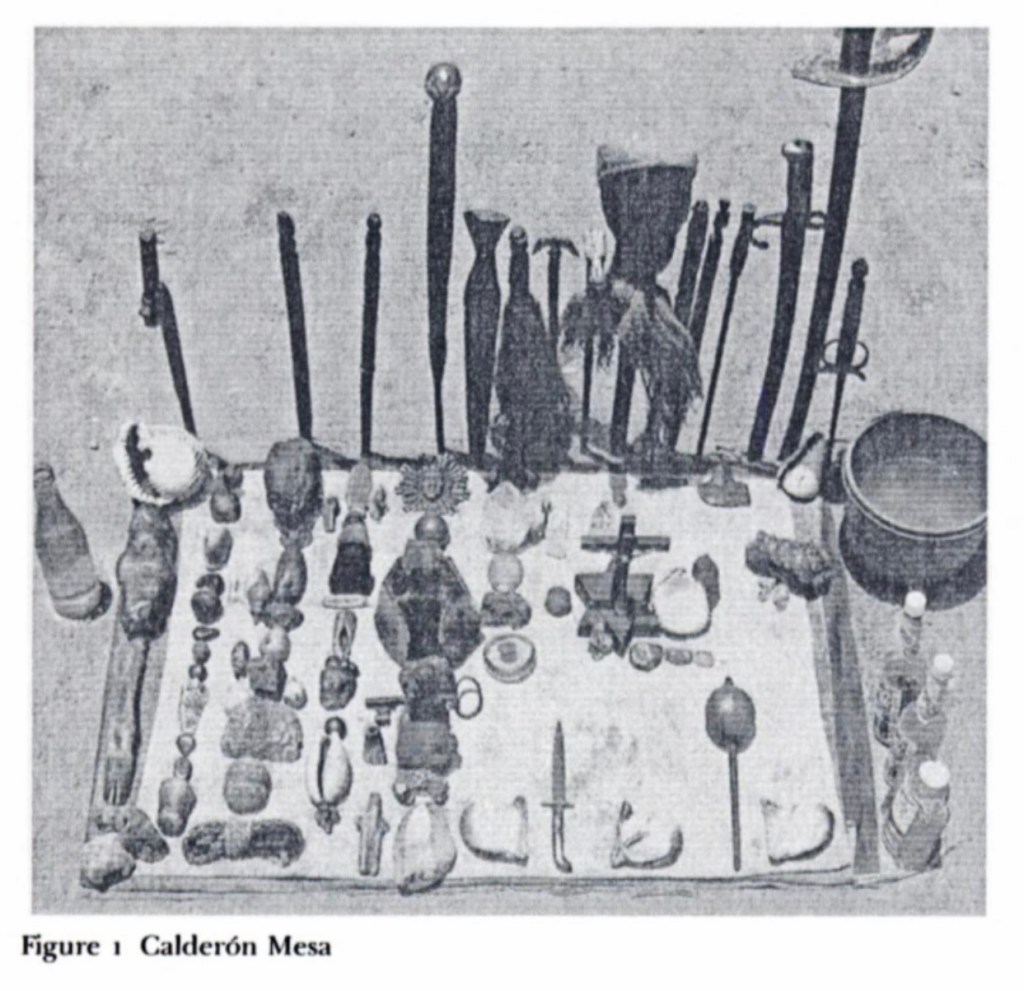
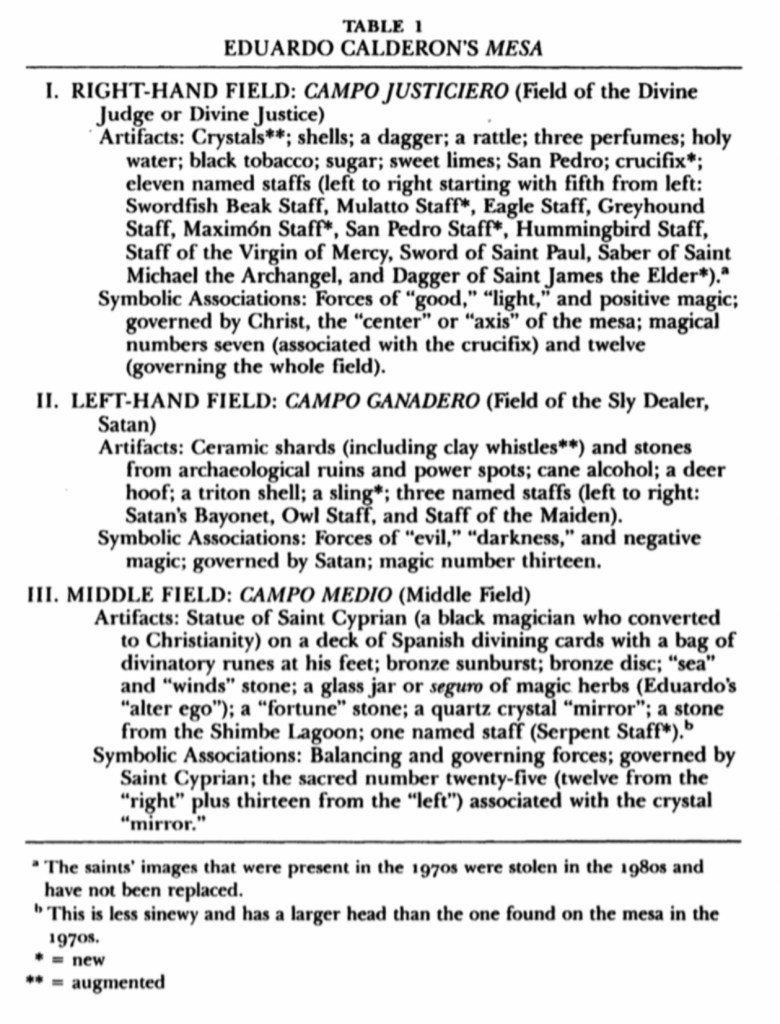
Eduardo’s mesa is spatially divided into two major (though un-equal) zones called campos (fields) or bancos (banks or benches), which are separated by a narrow third sector between them. He conceptualizes these divisions as a projection of his own inner curing power. Symbolically, they express a moralistic dualism of good versus evil (see Table 1). However, due to the symbolic role of the third or middle field, it could be termed a “balanced dualism,” probably best described as a dialectic of good and evil.
During a séance, which typically lasts from about 9:00 PM to 6:00 AM, the passage of time is measured by Eduardo through the performance of his ritual acts. These include: the reciting of Catholic prayers and an imitation of the Mass; the spraying of per-fumes; tunes (tarjos) whistled and sung to the beat of a gourd rattle; invocations (spoken and sung) of cuentas (power “accounts” or stories stored in mesa objects [artes] and made manifest in tarjos), as well as invocations of supernatural forces (encantos) located in mountains, lagoons, and pre-Columbian ruins (huacas); ingestion of San Pedro; limpias or “cleansings,” (i.e., rubbings with a selected staff); and periodic nasal imbibition of a mixture called tabaco in a ritual “raising” (levantada or parada). Each act has its own specific time and order in the overall ceremony.
Through the medium of rituals performed until midnight, Eduardo treats time in a linear fashion. This is done by what he conceptualizes as a power buildup. The session opens with Catholic prayers and invocations to the four cardinal points, interspersed by Eduardo spraying the mesa with perfumes. In the 1980s Eduardo added an exhalation or blowing of tobacco smoke in the four di-rections, as well as an invocation to the four associated power animals (i.e., north-buffalo/horse/dragon, west —jaguar, south-eagle, east—serpent/sun).5 Next is a series of songs and “raisings” to activate the crucifix and the three symbolic zones of the mesa along with their associated magical numbers. The sequence of activating or “charging” mesa sectors is as follows: crucifix and its associated number seven, Campo Justiciero (right) and its associated number twelve, Campo Medio (middle) and its associated number twenty-five. In the process of raising or activating the Middle Field, the Campo Gana-dero (left) and its associated number thirteen are also brought to life.
Midnight marks a period of transition in the night session. With the consumption of the San Pedro brew by all participants, the linear ritual acts which activated the dualistic ideological areas of good (right side) versus evil (left side) come to an end. This occurs at the same time that one twenty-four-hour day is ending and another beginning. As the curandero, the San Pedro brew, and the symbolic zones of the mesa are activated in both space (ritual artifacts and zones) and time (ritual acts and numbers) the stage is prepared for the second part of the curing session.
After midnight, Eduardo begins the actual curing portion of the séance. During this therapeutic division of the ritual the space occupied by the mesa artifacts is conceptualized as the realm of the “four winds” and the “four roads,” a veritable microcosmos replicating the interplay of forces in the universe. According to Eduardo, the “four roads” radiate out from the crucifix to the four corners of the mesa, dividing it into four triangles. Each triangle correlates with one of the four cardinal points, or “four winds.” This quaternary structure (four triangles) of the mesa during the second stage of the session contrasts markedly with the ternary structure (three fields) of the mesa during the first stage. However, despite that contrast, the second stage is an extension and refinement of the dualism expressed by the first stage. Although this is not as clearly verbalized by Eduardo as is the first phase of the ritual, it is implicit in his descriptions and strategic groupings of power objects (see Sharon 1978:62-72, 101-11, 159-74 for a detailed analysis of Eduardo’s mesa artifacts and associated rituals).
According to Eduardo, once the first stage of the séance produces a balanced power buildup, manifest in a “charged” mesa (including the San Pedro and the healer), this power is then ritually “discharged,”that is, applied in therapy. This occurs during the second part of the session, which lasts from midnight until 6:00 AM and consists of curing acts. Throughout the therapeutic portion of the séance, Eduardo treats time in a cyclical manner by repeating a standard series of curing rituals for each person participating in the session.
In effect, the sequence appears to be from right to left to right, as depicted below:
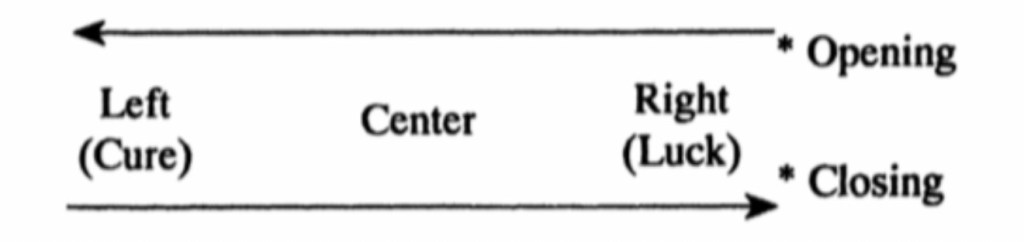
The goal of curandero therapy is to cure sorcery or soul loss. According to Eduardo, this goal is achieved through the therapeut application of the ritual “power” accumulated and “balanced” by the symbolic transformation of space and time that is delineated by a mesa during a curing session.
Sources;
Sorcery and Shamanism: Curanderos and Clients in Northern Peru by Donald Joralemon, Douglas Sharon
