





When anybody comes to the emergency department, the first thing that is done, is called the primary survey – looking at the basic parameters that can save lives, coded as CABCDE.
‘C’ stands for catastrophic haemorrhage. If the patient is bleeding significantly the first thing to do is to try to stop it, either by direct pressure or using a torniquet, a tight binding with a belt or a strap between the heart and the open wound. Sometimes the source of bleeding isn’t obvious, though, it maybe coming from somewhere hidden like the chest, abdomen or pelvis. The second check is ‘A’ for airway, to confirm there is no obstruction to the flow of oxygen to the lungs. Then come the lungs themselves, ‘B’ for breathing, to make sure the lungs can expand properly and provide oxygen to the body. The lungs could be bruised, or be compressed with blood or air, requiring a chest drain. The second ‘C’ stands for general circulation and a quick assessment of the blood pressure by feeling the pulses, while ‘D’ is disability, the most likely neurological disability caused by head injuries. ‘E’ stands for exposure – checking the rest of the patient and also understanding the temperature of the environment. To do this, it is important to remove as many of the patient’s clothes as possible, so that they can be examined front and back.
IEDs are improvised explosive devices used against coalition borders in Afghanistan. The Taliban fighter came in, he operated on him, and his life was saved. He (Dr Nott) explains that he doesn’t get to choose who to work on, he tries to intervene to save the life of the person who is in desperate help.
He does, though rationalise by thinking that maybe the fighter’s outlook might change on someone like him, a Christian doctor saving his life which some might find naïve. He recounts that he was taught by the best pilot, Peter Godwin, holds a flight instructor rating. He also ferried a group of British doctors in Scotland who would climb Mount Everest in 2007.
After a woman who he knew died on the operating table smiling. He began missing lectures and clinical work, and ended failing the end-of-year pathology exam. During the microbiology resit, rather than discussing about bacteria and viruses, the examiner talked to him about why he was having to resit the exam. All his anxieties came out in those twenty minutes, was told to his amazement that he would pass, and that to having answered only a simple question of gas gangrene. The last year of clinical training was tough, with many hours spent studying late into the night, on top of the clinical work on wards. But it paid off, he graduated with distinction in medicine and paediatrics in his final exam. Sometimes a distinction is drawn between those in ‘medicine’ and those in ‘surgery’, to show the difference between doctors who diagnose and prescribe, and those who diagnose and operate. He already knew that the technical aspects of surgery appealed more to him than diagnostic puzzles and that he inherited a good pair of hands from his orthopaedic surgeon father.
MISSION 2#
TO SARAJEVO
GOVERNING BODY; MSF
LOCATION – BOSNIA AND HERZEGOVINA
As part of his preparation for work overseas he had already been on a two-week course with the British Red Cross, to get accredited as a volunteer. When he rang the ICRC (International Committee of the Red Cross), they informed him that he would have to go for 6 months, and this meant letting down his patients and colleagues somewhere. His surgeon friend told him that there was another way, Médecins Sans Frontières offered shorter placements – even of only two or three weeks, provided MSF accepted you as a volunteer, it was up to you to decide how to go long for. So, our vascular consultant rang MSF and then went on an interview with them.
By the end of 1993 the country was deep into a brutal and civil war. The Bosnian capital, Sarajevo, had been besieged and blocked by the Bosnian Serb army since May 1992. For a cosmopolitan, outward-looking city, which only eight years had hosted the Winter Olympics, the siege was unprecedently traumatic.
Perhaps this is the moment, the place to get involved? He justifies.
He went to see his boss at Charing Cross and explained that he needed to go to Sarajevo. ‘And where do you think you will get someone to do your job it’s Christmas!’ He said red faced and angry. Our hero made a phone call, ‘Eric, I will pay you £2000 of my own money will you do my locum?’ Eric Grocott was a very experienced Senior Registrar from Australia. He responded with an ‘All right mate.’
Just before Christmas 1993 He packed some warm clothes and a sleeping bag and left his comfortable flat in Hammersmith to fly to Zagreb, the capital of Croatia, the newly independent country to the north of Bosnia and Herzegovina. He went straight to the MSF office, where he found a contingent of British plastic surgeons and Belgian MSF staffer who briefed us on the logistics of our trip.
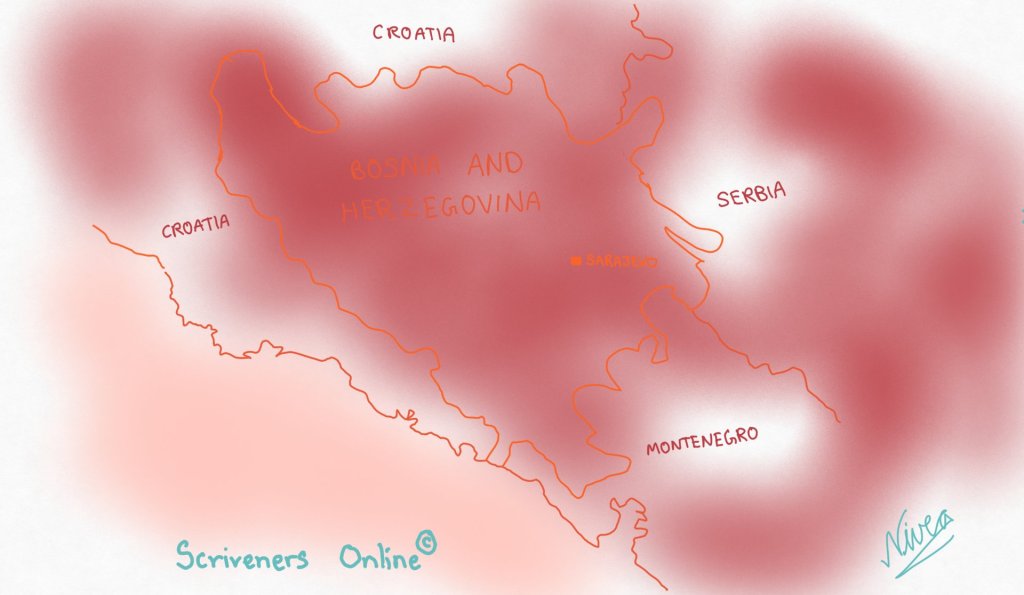
They poured over a map of the region while the MSF logistician drew on it to show us the front lines around Sarajevo, a city in a fairly narrow valley surrounded by hills and mountains, and told us that the Serbian army controlled the high ground to the south. He explained how to use the walkie-talkies we wound be issued with, and the correct radio terminology – something our hero’s flying experience had prepared him for. Many things were new and strange; like being told how to wear our flak jackets and helmets, warnings about the dangers one would face meaning there’s an absolute ban on one’s movement independently, the different types of artillery being used on that city; and the kinds of injuries one might expect; at the expense of the constant threat of the snipers.
He could hardly believe that he’d be in the middle of all this at the end of the day. There was much form-filling to be done, and disclaimers to be signed, and they were also told that they could back out if they were having second thoughts about going unarmed into one of the dangerous places in the world. Dr Nott thought about this and the outcome was a sleepless night before arriving to Sarajevo. But he also says that the sleeplessness was from the excitement as much as the anxiety. Before they left Zagreb, they were issued with credit card sized UNHCR passes – proof that we were working under the auspices of the United Nations High Commissioner for the Refugees. The cards were more important than their national passports in some ways. As a civilian, one couldn’t get in or out of Sarajevo without one.
One night about two weeks into the mission, a youth of sixteen years was brought in. A large fragment was in his abdomen, Sarajevo at that time was under high bombardment, and the metal fragments from these projectiles produced similar injuries to that of a bullet, but often larger and more destructive. The patient was bleeding so badly that he had low blood pressure and high pulse rate, they had limited resources and were freezing. They had two choices; either operate and save his life or watch him die. There were four of them in attendance; the vascular surgeon, an anaesthetist, a scrub nurse and an assistant.
Once he was under anaesthetic and being infused with only one pint of blood the team had, he opened his abdomen. The operation in which the surgeon examines all parts o abdomen and pelvis, with your eyes and hands; the solid and the hollow organs is called a laparotomy. It also involves making decisions such as whether or not to expose the aorta. The fragment punctured his inferior vena cava, the silver of the metal was still there, partially stemming the bleeding. His heart was pounding whether he would be able to control the bleeding after removing it and he knew he needed to pack the wound immediately. As he gently removed the fragment, a fountain of blood spurted out of the torn blood vessel, he grabbed a big gauze from the tray and pressed it on the gushing area.
While he was thinking about what would be next, there was a sudden crash and the whole building shook. It felt as if the structure was going to collapse any moment and it was also pitch black. He could no longer see his patients or colleagues. He was still pressing the swab on the the patient’s IVC and with his other hand he could feel the aorta, he could make out as in his line of profession, what the blood pressure is like but just palpating the aorta, this one’s was slipping. He squeezed the aorta with his fingers to try and occlude it, maintain the blood pressure to his heart and brain. ‘Packs, packs!’ he shouted. Minutes passed with an eerie silence filling the room, he waited and waited, the boy’s IVC getting weaker and weaker, ‘Hello! Hello! I need lights here! Anyone there?’
He called and called and to avail the boy had died and he knew it. He was a loss at what to do, and had just waited with the warm blood becoming colder, some minutes later the lights began to flicker, and it was back on, he looked around the theatre; there was no one; the entire theatre team had fled to take cover. The poor boy had lost three to four litres of blood; he should’ve survived maybe the old woman before didn’t stand a chance but he should’ve survived. Every now and then, the hospital would be engulfed in complete darkness, often in the middle of the night, a man would come into the operating theatre with a wheelbarrow full of five or six car batteries but this time it wasn’t the case.
No one had said to him, ‘David, we’re going, you’ve got to come too.’ He was left in utter despair. The importance of self-preservation was brought onto him a couple of times like this on this first mission.
Source:
War Doctor-David Nott (2019) 2020 Edition

Leave a comment