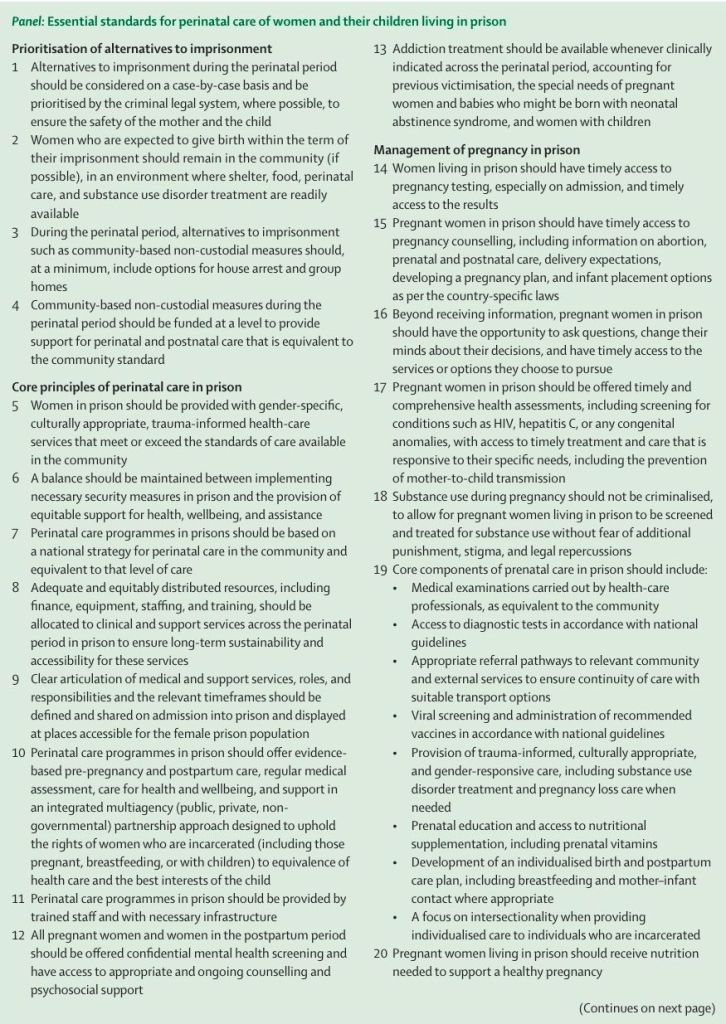
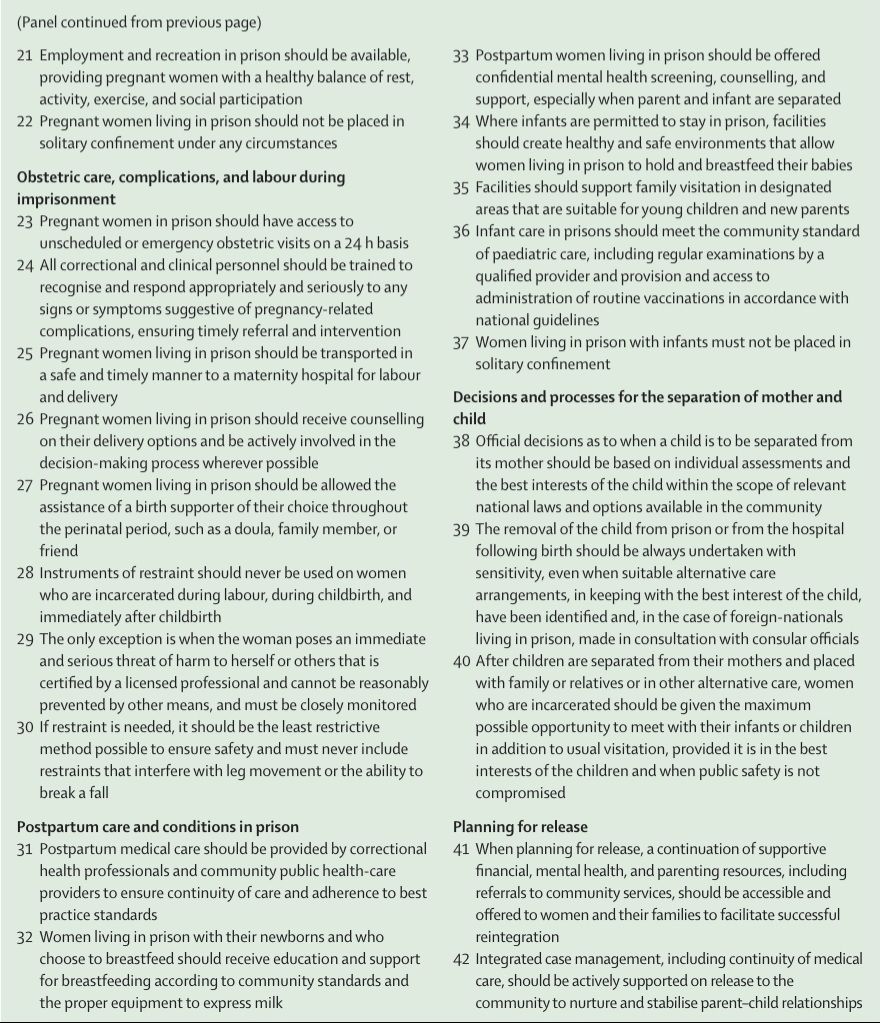
Essential standards for perinatal care of women and children living in prison
The female prison population continues to rise, with prisons worldwide failing to meet international human rights standards. Many are overcrowded, poorly resourced, and unsafe, especially for women. Women in prison are an obstetric group at high risk, with deficits in perinatal care leading to preventable maternal and child morbidity and mortality. Mother–child imprisonment and mother–child separation can have substantial intergenerational health and social consequences. In this Viewpoint, we present essential standards for perinatal care of women and children who are incarcerated, aligned to human rights obligations, prioritising alternatives to imprisonment, and where custodial sentences are applied, emphasising essential core best practices in prison (inclusion of prisons in national maternal health strategies, resourcing of prison facilities, services, staffing, and medical competencies, comprehensive medical management of pregnancy, obstetric and postpartum care, and release planning). To ensure the rights of women and children in diverse contexts are upheld, standards should be enforced through independent inspections, clinical audits, and integrated public and prison health monitoring of perinatal health outcomes.
The global prison population has remained steady, at 11·5 million in 2025.1 However, the proportion of women who are incarcerated is continuing to rise at an alarming rate.1,2 More than 733 000 women and girls are incarcerated worldwide, with the female prison population increasing by 57% since 2000.1,2 Steep increases are observed in South America (Brazil), Central America (El Salvador and Guatemala), and southeast Asia (Cambodia and Indonesia). The USA has the highest number of women living in prison (approximately 174 607) in the world.2 Incarceration rates of women are generally underpinned by punitive responses to drug-related offences, offences directly or indirectly related to gender-based violence, and nonviolent, low-grade offences, often linked to poverty.1–3 Women who are incarcerated often have complex and substantial health needs, including psychiatric illness, substance dependence, and trauma,1,4 and might experience pregnancy and motherhood in prison.5–7
Despite recognised international human rights norms and obligations regarding the treatment of all people who are incarcerated (eg, UN Standard Minimum Rules for the Treatment of Prisoners 19 and UN Rules for the Treatment of Women Prisoners and Non-Custodial Measures for Women Offenders20), many prisons worldwide fail to meet such standards and are overcrowded, poorly resourced, and unsafe, especially for women.1,21,22 National Preventive Mechanisms under the Optional Protocol to the Convention Against Torture and other Cruel, Inhuman and Degrading Treatment or Punishment (OP-CAT)23 and UN treaty body committees routinely document neglect and rights violations concerning the situation and treatment of pregnant women and mothers worldwide who are incarcerated.14
Recognising these underlying drivers of disadvantage is essential to understanding the heightened vulnerability of pregnant women in detention and the need for comprehensive, rights-aligned reforms. There is growing international consensus that imprisonment of pregnant and postpartum women is rarely justified and is inconsistent with human rights obligations and the requirement to prioritise the best interests of the child.11–15,17,18 Decongestion measures, including through greater application and prioritisation of alternatives to imprisonment, and immediate, evidence-informed reforms to respect, protect, and fulfil maternal and paediatric health rights and outcomes in prisons are crucial.3,4,7,11–13,15,17,18,24,27–29 Evidence regarding communitybased alternatives remains scarce, yet what is available highlights their potential to reduce harms and strengthen continuity of perinatal care.12,14–17 Combined with identified risks associated with perinatal care in prison, including preventable maternal and neonatal morbidity and mortality, lack of emergency obstetric access, unsafe conditions, and trauma-exacerbated environments, these factors support the argument that non-custodial measures should be the presumptive response, with deprivation of liberty used only when no safe alternative exists.
By encouraging equivalency of maternal and paediatric outcomes, in addition to care that is at least equivalent to that available in the community, and implementing integrated health care spanning community and prison, maternal and child health can be better protected and ensured. Greater investment in community health care, integration of lived experience, and monitoring of perinatal outcomes through independent oversight mechanisms are essential to reducing preventable morbidity and mortality among mothers and infants affected by the criminal legal system. Clinical audits and independent inspection mechanisms including those created by OP-CAT are crucial to monitoring prison standards and ensuring access to and quality of provided health care. Monitoring efforts help to ensure compliance with human rights and accountability and play an important part in supporting and ensuring positive perinatal health outcomes for mothers and children living in prison.14,22,24,28,29
In this context, the work of non-governmental organisations (NGOs) in helping to implement the essential minimum standards of perinatal care for women and their children living in prison systems is of particular importance. For example, the international NGO Health through Walls operates globally to strengthen health care in prisons, by partnering with correctional systems in low-income countries to improve continuity of care, including access to medicines and diagnostic equipment, capacity building for support staff, and developing sustainable prison health systems. Their model integrates public, maternal, and paediatric health approaches with human rights obligations by working to address many of the gaps in implementation of such essential minimum standards of perinatal care and management in prisons.
Sources;
Lancet Public Health 2026; 11: e197–201
Vol 11 March 2026
