Every year, more than 5 million patients undergo surgery in the UK National Health Service (NHS), and about 100 000 die within 90 days of surgery.1 It is now widely accepted that older patients with multiple long-term conditions account for a disproportionate number of deaths after surgery.2–4 These high-risk patients have worse postoperative outcomes, not because of technical failings in anaesthesia or surgery, but because of acute medical complications such as myocardial infarction, pneumonia, and stroke.5,6 These complications result from the interaction of existing long-term medical conditions, older age, and the inflammatory response to major surgery.7
Efforts to improve outcomes for patients at high risk of poor outcomes after surgical treatments (hereafter termed high-risk surgical patients) have typically focused on specific patient groups, for example, those undergoing emergency abdominal surgery.8,9 However, high-risk surgical patients have a wide range of diseases, which need different surgical care pathways. Despite this variation, the great majority of these high-risk patients subsequently receive their surgery within the same preoperative, perioperative, and postoperative services, which they also share with a much larger number of younger, healthier patients. These services include the same operating rooms, post-anaesthetic recovery units, and hospital wards; with the same nurses, anaesthetists, and other health-care professionals.
System-wide solutions are therefore required to identify high-risk patients being treated within health systems and deliver the complex individual care they need to achieve a good surgical outcome. These solutions could improve the value of the care provided, since costly interventions that might benefit high-risk patients could be focused on them rather than being widely applied. A shift towards value-based health care, rewarding patient experience and outcome, rather than the volume of procedures performed, might also ensure better alignment between patient wishes and care provided.10
Initiatives such as the UK Centre for Perioperative Care have been established to provide this multiprofessional approach, including representation from both community and hospital services. Although these system-wide health policy initiatives have a valuable impact, they are ultimately limited by our understanding of the number of high-risk patients who undergo surgery, their healthcare needs, and subsequent long-term outcomes.
The number of surgical treatments provided by the NHS continues to rise steadily, while the NHS surgical population is now ageing faster than the background population.1,11 A continued rise in numbers of high-risk surgical patients might outstrip measures to improve their care. The aim of this study was to describe the size, demographics, and long-term outcomes of the UK population at high surgical risk. This evidence is urgently needed to inform the health policy change required to ensure optimal outcomes for these patients.
This high-risk population has a high mortality: one in seven will die within 90 days; one in four will die within 1 year after surgery, and four in ten will survive the next 5 years. These surgical patients in the high-risk group stay much longer in hospital, accounting for more than half of all bed days used by surgical patients. They also account for a third of emergency hospital readmissions after surgery. While procedure-specific risk and admission type have a role in surgical outcomes, other risk factors for this patient population are age (>70 years), multiple long-term disease, and frailty. This population is likely mirrored in other high-income nations and therefore represents a global challenge to health-care policy and delivery.
The most widely cited paper describing the NHS high-risk surgical population was published in 2006, and it described an annual population of 166 000 patients.29 In our current study, we identified a larger population, with a lower overall risk of short-term death. This change is primarily because of the substantial growth in surgical procedure volumes for high-risk patients over the intervening time period, although the current study also takes a more inclusive epidemiological approach. We found that patients with multiple long-term disorders were more likely to be in high-risk groups.17 The growing number of people living with multiple long-term disorders might be an important reason why a quarter of high-risk patients died in the year following surgery. Many clinicians will argue that surgery is an incidental event in this context. However, as the purpose of surgical treatment is to offer the patient a greater quality of life, quantity of life, or both, it is essential to consider the effect that high-burden treatments can have in the last year of life.
The overall decrease in postoperative mortality for all risk groups is important and suggests standards of patient care are improving despite the growing volume of high-risk cases. Nevertheless, public expectations of health-care continue to rise, and improvements in care over time have not been sufficient to resolve the problem of poor outcomes for high-risk surgical patients. Consequently, it is challenging for the NHS to deal with the scale of the current high-risk surgical population and to be prepared for the likely continued growth in this population over the next 20 years. While our data focus on the NHS, high-risk surgical populations exist in other high-income nations and likely face the same challenges. Identifying high-risk populations may serve as a target for focused improvements, for example, in randomised trials of perioperative interventions, or for prospective observational studies to understand this phenomenon more clearly. The poor outcomes experienced by high-risk patients also have wider health system implications such as the requirement of in-hospital beds for prolonged periods of time. If interventions could be identified to improve outcomes for this relatively small patient group, then they could free up resource for the broader population of patients awaiting care.
The findings are particularly important in the context of shared decision making about surgical treatments.12,31 For many decades, 30-day mortality has been the most used measure of the success of surgical treatments. While short-term mortality might provide a useful measure of harm, it is clearly not the success measure patients are focused on.32 Our data show that one in four high-risk patients who underwent surgery died within 1 year compared with one in 20 of the overall surgical population. Many high-risk patients survive severe complications only to be left with a substantially reduced quality of life.33–38 However, while our data show many high-risk patients have poor outcomes, it is not possible to predict before surgery which patients would experience better outcomes with conservative (nonsurgical) care.
In conclusion, between 2015 and 2019, 300 000 high-risk NHS patients received a surgical treatment annually; of whom one in seven died within 90 days, one in four within 1 year, and two in three within 5 years. These patients are typically aged over 70 years, have multiple long-term diseases, and are likely to be frail. The high-risk surgical population is small compared with the overall NHS surgical population (~9% of all procedures) but accounts for over half of NHS perioperative resources. This will create an ever-increasing health-care policy challenge, which will likely grow steadily over the next 15 years and is unlikely to be confined to the UK. A renewed policy and research focus to improve outcomes will benefit both patients and the wider health-care system. A society-level debate is needed about the risk and benefits of surgical treatment for older high-risk patients, and whether surgery is always the best option for those patients readily identified as high-risk.
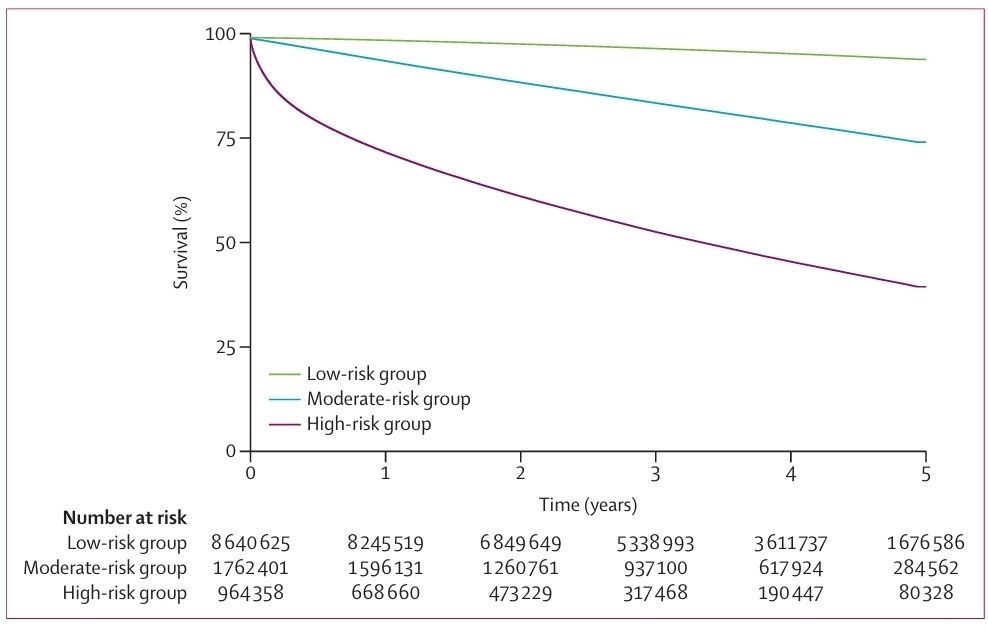
Time is recorded in completed years following index surgery. Line thickening is censoring to final date of outcome capture. The appendix (p 7) shows cumulative survival probability. Log-rank test p<0·001.
Sources;
Lancet Public Health 2026; 11: e197–201
Vol 11 March 2026
