What has been the trend in hospital-based shootings over the past 25 years in the US?
Introduction
Firearm-related violence is a concern in the US, with the Centers for Disease Control and Prevention reporting more than 48 000 firearm-related deaths in 2022.1 Workplace violence in health care is also a concern, with US health care workers being 5 times more likely to experience an injury from violence than workers in any other industry.2 When workplace violence involves the use of a weapon, fatal injuries can result.2 Health care spaces are not weapons free, with a recent systematic review and meta-analysis finding a concerning prevalence of weapons in health care, ranging from 1.6% among individuals entering the emergency department to 24% among patients with major trauma who were hand searched.3 These rates are alarming given the risk weapons pose to health care staff.
Outcomes
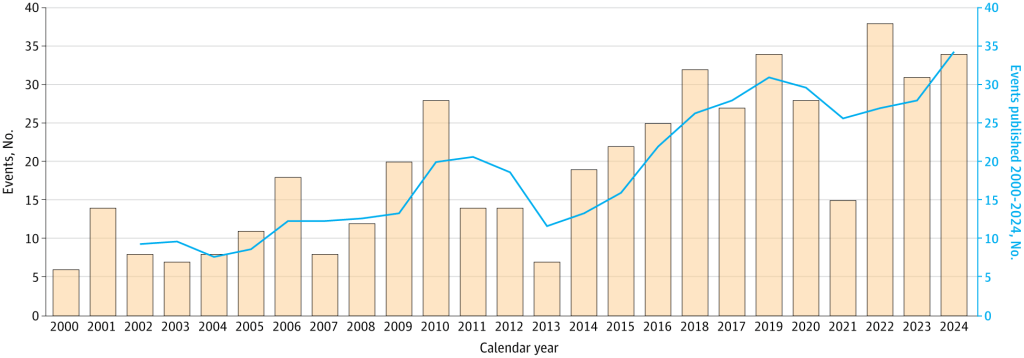
Violence in health care has increased in recent years.2,4 While studies conducted from 2000 to 2011 and 2012 to 2016 have identified a rising incidence of hospital-based shootings, there has yet to be a comprehensive updated analysis.5,6 Thus, despite growing concern, the current state of these events in the US remains poorly understood. Our study objective was to categorize US hospital shootings from 2012 to 2024 and incorporate prior published shooting events between 2000 and 2011 to assess trends in shootings over a 25-year span.5
Discussion
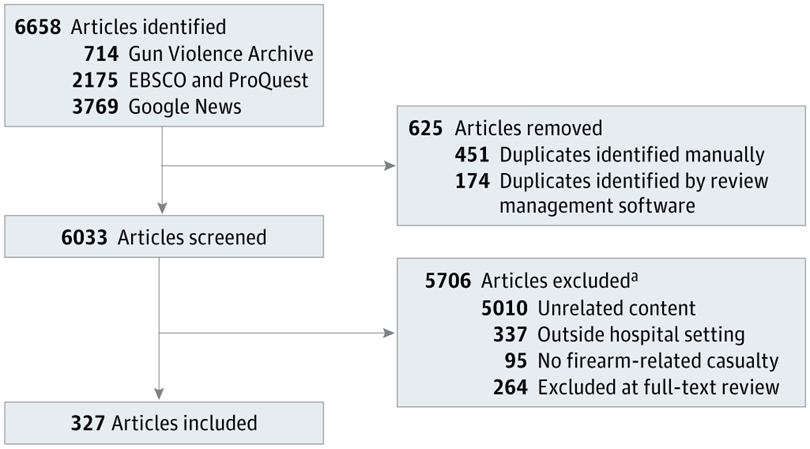
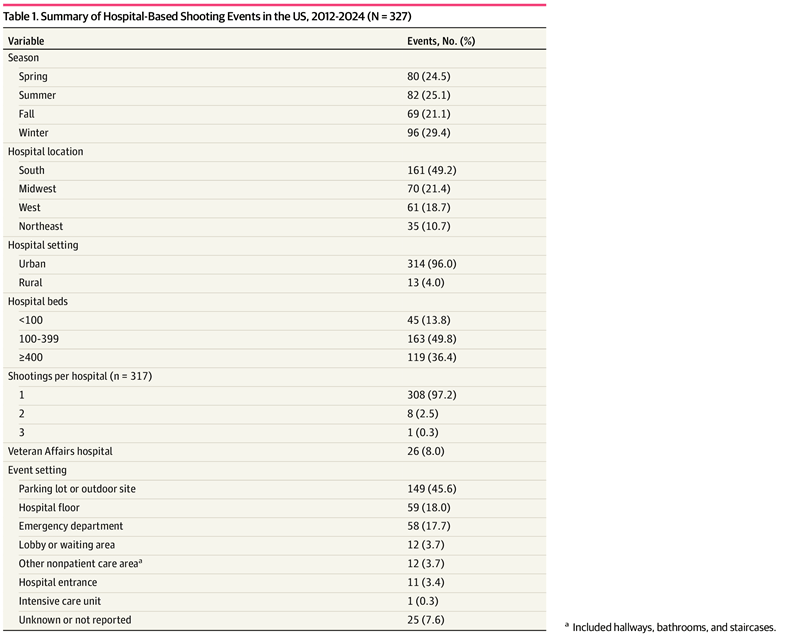
This systematic review found that hospital-based shootings in the US have continued to rise over the past 2 decades, with 327 shooting events (5.2 events per year per 1000 hospitals) identified between 2012 and 2024, more than double the 154 events (2.2 events per year per 1000 hospitals) previously reported from 2000 to 2011.5 Across all 25 years, the US saw an increase in hospital shootings of more than 6% per year. From 2012 to 2019, hospital-based shooting fatality rates closely tracked national firearm fatality trends, with a relatively strong year-to-year correlation, suggesting that shootings during this period may have at least partially reflected broader firearm violence in the US.13,340 However, this correlation weakened from 2020 to 2023, during which time national firearm fatalities increased while hospital-based firearm fatalities decreased, particularly in 2021. This finding may be the result of COVID-19 pandemic–related reductions in patient volumes and strict visitation policies, limiting opportunities for violent encounters. Overall, these findings suggest that while hospital-based shootings may reflect national firearm trends, they may also be influenced by health care–specific factors.
The southern US experienced the highest total number of shootings and per-capita shooting rate, consistent with previous findings from 2000 to 2011.5 This finding mirrors overall US firearm mortality data, with Mississippi, Louisiana, and Alabama consistently leading the nation between 2014 and 2024 in firearm mortality rates per 100 000 total population.341 Additionally, a study from 2022 found that the US South had the highest percentage of firearm-related hospital admissions of all regions, accounting for more than 40% of all admissions, while also having the weakest firearm regulations.342 We found that large hospitals (≥400 beds) continued to experience the highest rate of shootings, consistent with previous findings from Kelen et al.5
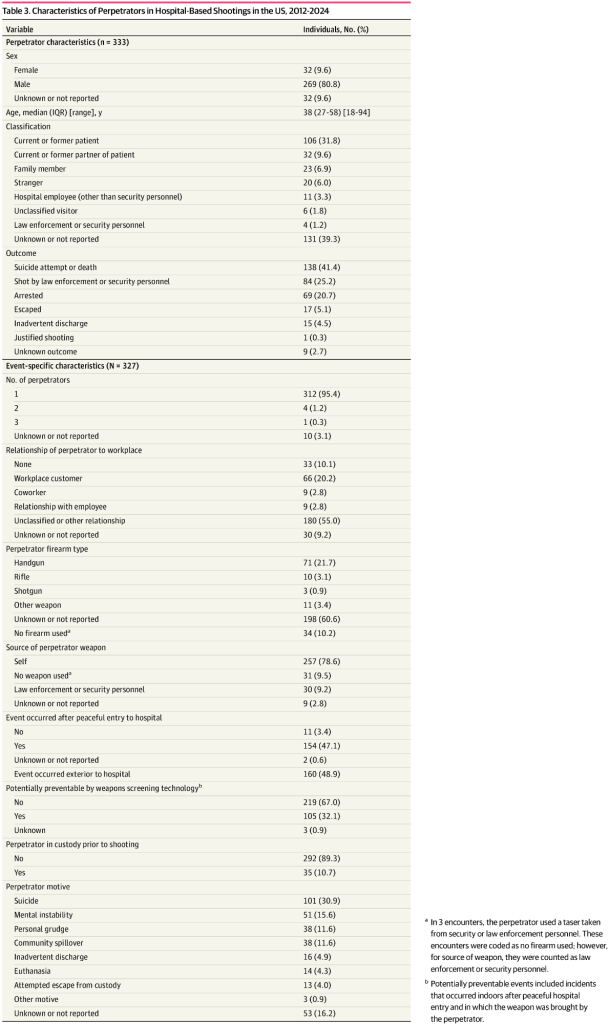
Of note, suicide was identified as the perpetrator’s motive in nearly one-third (31%) of events, and 41% of perpetrators eventually attempted or died by suicide after the event. This finding represents an increase from the 21% motivated by suicide in the prior analysis5; however, it does reflect data from the Federal Bureau of Investigation that 34% to 40% of active shooter incidents between 2000 and 2019 resulted in the shooter dying by suicide.5,343,344 Our finding of a rising motive of suicide among hospital-based shooters may reflect larger societal patterns as the total age-adjusted suicide rate in the US increased from 10.4 per 100 000 population in 2000 to 14.2 per 100 000 in 2022, with firearms the most common method used in suicides (>50% in 2023).345 Notably, many suicide-motivated shootings in our study were uniquely tied to the hospital environment, including individuals intentionally ending their life in the hospital with the explicit goal of organ donation or those dying by suicide after receiving upsetting health information.
While the majority (79%) of shootings involved firearms brought by the perpetrator, 9% involved firearm diversion from law enforcement or security personnel, comparable with findings from previous analyses.5,6 Also similar to prior literature, individuals in law enforcement custody were disproportionately involved in emergency department shootings, and these events accounted for the highest proportion (59%) of firearm diversions.5 Although armed presence is expected among law enforcement officers, and to a lesser extent among hospital security personnel, our findings suggest that these weapons could become sources of harm when overtaken by individuals with malintent. Our findings related to firearm diversion highlights the importance of ongoing training for armed hospital security and law enforcement personnel and support the development and use of devices to secure service weapons, such as high-retention holsters.346
Our analysis showed that nearly one-third of shootings were potentially preventable by weapons screening technology, as many perpetrators entered facilities unimpeded while carrying firearms in holsters or bags that could have been detected with screening. Nationally, weapons screening in hospitals remains inconsistent. A survey of hospital security directors and administrators found that 48% reported metal detectors at some of their hospital entrances, with comprehensive coverage of all entry points far less common.347 This finding differs from other high- volume public settings, such as airports, sporting arenas, and government buildings, in which advanced weapons detection technology is often used. When used, screening technology is effective at finding weapons; however, it has notable drawbacks, including cost, staffing, space requirements, and queue length,3,348 3,348 Hospitals equipped with this technology have been shown to confiscate weapons at 5 times the rate of those without, while increasing reported perception of safety among patients and employees.349-351 Overall, our findings suggest that the introduction or expansion of weapons screening processes may represent one of the most reliable opportunities to prevent firearm incidents in the hospital setting.
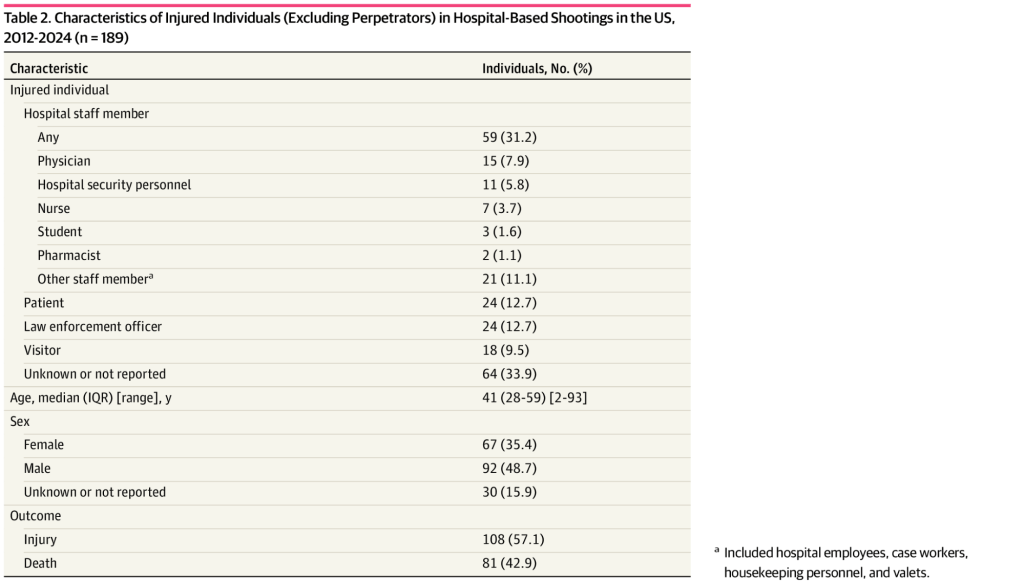
We recognize that although hospital-related shootings constitute a small fraction of national firearm vi- olence, their impact could be profound.340 In addition to the immediate injuries and fatalities sustained by staff, patients, and visitors, these events may produce an enduring psychosocial impact on communi- ties and operational consequences for institutions, so much so that training for these events in the form of active shooter drills has been shown to be traumatizing to health care staff. 352 Prior studies of workplace violence in health care, of which shootings represent one of the most extreme manifestations, have shown a broad impact on staff, including depression, post- traumatic stress, and job attrition, leading to a de- cline in patient care quality and overall workforce capacity,353,354 Hospitals may also experience reputational harm and increased financial costs associated with security infrastructure and litigation after a shooting. Overall, these events erode both the ability and perception of hospitals to function as secure and trusted care environments in the communities they serve.
Conclusions
This systematic review found that hospital-based shootings in the US have increased steadily over the past 25 years, representing a unique intersection between broader national trends in workplace and firearm violence. Our findings highlight that large hospitals, those in the US South, and those in urban communities are particularly at-risk settings, with a growing proportion of incidents driven by suicide attempts and deaths. These results underscore the need for hospital-specific prevention strategies, including consideration of weapons screening processes, alongside broader societal and community efforts to address rising firearm violence.
Source;
JAMA Network Open
Vol 9 Number 6
