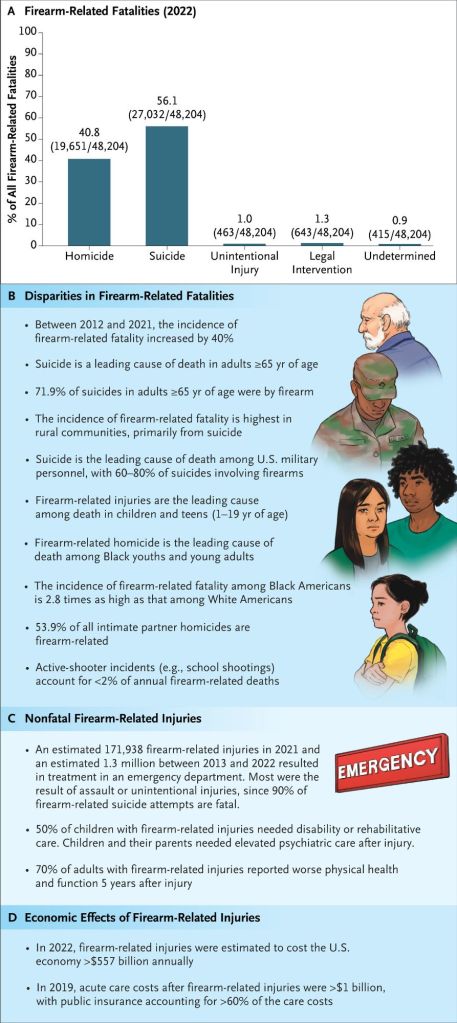
Firearm availability is closely linked to multiple firearm-injury outcomes.34-36 In 2022, 45% of US households reported owning firearms, and two thirds of those reported having multiple firearms.37 Household firearm ownership is associated with increased risk of firearm-related adult homicide and suicide,35,38–40 adolescent firearm suicide,41 and unintentional firearm-related injury regardless of age.36 Almost 60% of homicides involving intimate partners are firearm-related,44 with the risk of femicide increasing by a factor of five when the male perpetrators have firearms.42 In addition, in 80 to 90% of teen suicides by firearm, unintentional firearm-related deaths in children, and school shootings perpetrated by teens, the firearms were obtained from the home of the child or teen or from a relative’s home.4,43
Firearm-related injuries are an urgent health crisis in the United States, with firearm-related deaths surpassing deaths from motor vehicle crashes in 2017.1 In contrast to other conditions for which clinicians have evidence-based solutions to reduce harm, the 25-year gap in federal research funding2,3 halted substantial advances in the science of firearm-related injury prevention. Yet renewed funding and emerging science continue to highlight the critical role clinicians have in prevention efforts.2,3
The lack of research has resulted in a generation of clinicians currently lacking the training necessary to implement the solutions generated by recent science. As a result, despite clinicians recognizing the need for prevention and agreeing that prevention of firearm-related injury is within their scope of practice,13 few deliver evidence-based interventions even though their patients find such measures acceptable within the context of clinical care.14 This lack of training is compounded by a shortage of adequate health care infrastructure necessary to support the integration of useful approaches into practice. Clinicians note multiple barriers, including a lack of knowledge, guidelines, time, clinical support, and reimbursement, as well as a fear of offending patients or encountering legal trouble.15-17
Clinicians routinely provide harm-reduction measures and anticipatory guidance for a range of complex health issues (e.g., substance use and vaccination), capitalizing on available evidence, their relationships with patients, and their community standing to promote health and safety. Although gaps exist, there remain opportunities to improve the current standard of care for the prevention of firearm-related injury. In this article, we review clinical approaches to prevention, ranging from ones implemented within individual clinical encounters to ones advanced by health care leaders within the systems and communities they serve.
Similar to other behavioural-health issues, the primary clinical approach to patients at an increased risk for firearm-related injury is prevention counseling to increase safety behaviours.
In the absence of guidelines from health authorities, researchers14,19–22 have advocated for pragmatic approaches that embed anticipatory guidance regarding secure storage and safety practices within routine primary care encounters (e.g., wellness examinations) while reserving more intensive prevention efforts (e.g., lethal-means counseling) for patients at increased risk for specific outcomes (e.g., firearm-related suicide). This approach also recognizes that risks are not static and may change as a patient’s clinical, household, or firearm-ownership status changes.19
Although defining the most effective prevention strategies remains an active research area,3,20 consensus recommendations have emerged 2,14,19,20,23 to guide clinical practice.
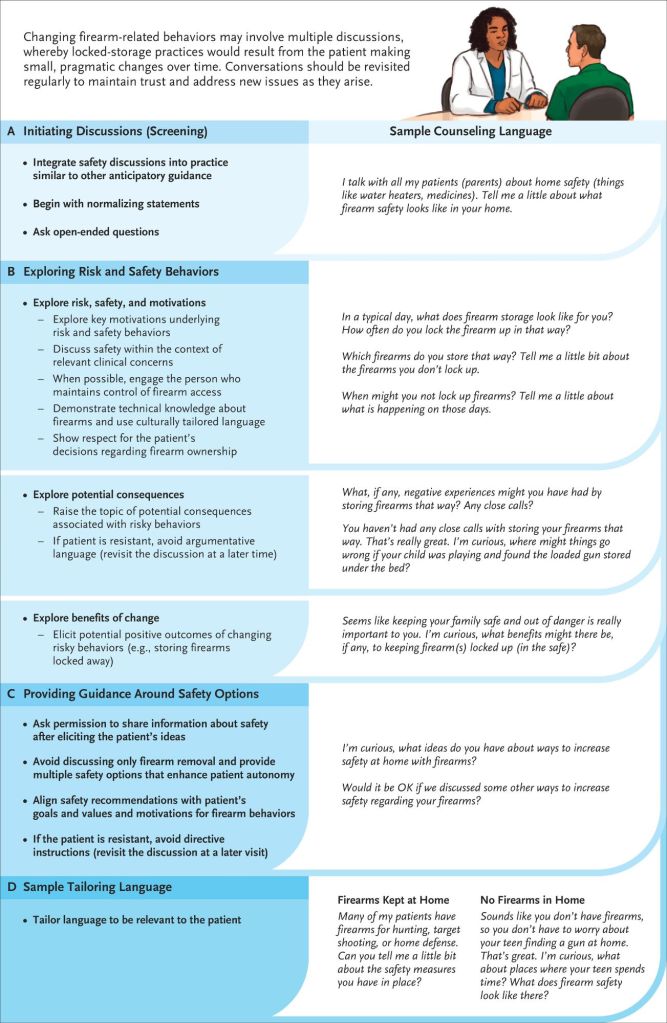
First, national organizations2,24 have advocated that clinicians integrate firearm safety discussions into their practice in ways that parallel the anticipatory guidance they provide regarding other risk behaviours (e.g., smoking). Incorporating firearm safety as a routine component of clinical care normalizes the topic for patients and the health care team, thereby reducing stigma around having such discussions in a clinical setting.
Second, as is true of other sensitive behavioural issues about which clinicians provide guidance, patients are more receptive to safety counselling — and clinicians are more likely to deliver such counselling — when the clinicians have technical knowledge about firearms, use language tailored to the patient’s cultural norms, show respect for the patient’s firearm-ownership decisions, and discuss safety within the context of relevant clinical concerns.14,16,19,25,26 In line with this approach, patient-centered counselling methods (e.g., motivational interviewing) that emphasize nonjudgmental, nonconfrontational, and apolitical discussions have greater acceptability and efficacy than directive counseling methods.17,27–29.
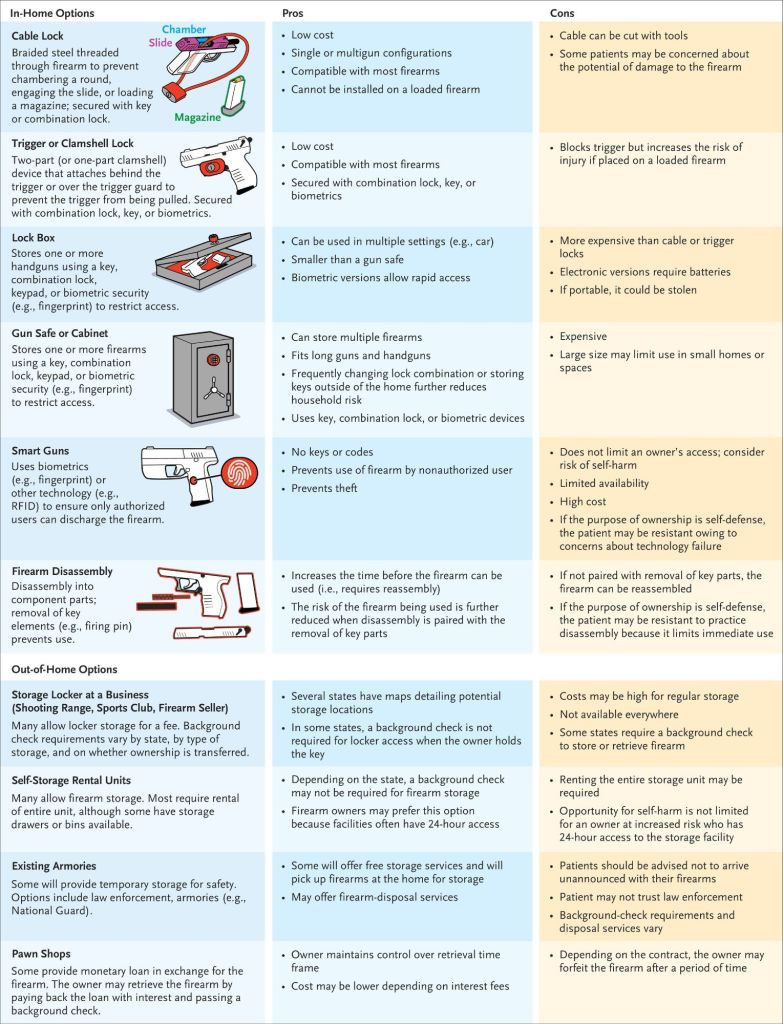
Third, counselling is most effective when clinicians align safety recommendations with patients’ motivations for firearm ownership and carriage (e.g., self-defense), as well as their goals and values. Although disposal of firearms provides the greatest level of risk reduction, this step may not fit within a patient’s values, and discussions in which clinicians recommend removing household firearms as the only safety recommendation evoke the most resistance30,31 and are largely ineffective.30,31 Consistent with principles regarding behavior change, routine discussions should emphasize multiple harm-reduction strategies that maintain patient autonomy. This approach should mirror substance-use counselling, in which attaining long-term behaviour modification frequently builds from small, pragmatic changes that patients identify as ones they are capable of enacting to reduce risks. Similarly, changing firearm-related risk behaviours may involve multiple discussions, with clinicians supporting any positive actions that the patient feels empowered to implement to reduce risks. Although this approach may not achieve all the recommended safety outcomes initially, it avoids evoking patient resistance and eliminating future opportunities for discussion. As with other health issues, in the absence of imminent risk, clinicians encountering resistance should modify their approach by identifying barriers to counselling, establishing patient safety goals, and attempting to reengage the discussion at a subsequent visit.
Finally, it is important to note that despite previous challenges, counselling is protected by the First Amendment, and no current state or federal laws prohibit clinicians from discussing firearm safety when it is relevant to the health of their patients or others.15 Although this protection extends to clinical documentation, patients may be resistant to safety discussions if information about their firearm ownership or access is recorded in the medical record.25 Given that this information is not critical to counselling, omitting ownership status and details (e.g., number and type or firearms) from documentation may lessen resistance.32 Of note, although the Affordable Care Act includes language prohibiting organizations from requiring the collection of patient firearm data for health and wellness programs, the Department of Health and Human Services has noted that this prohibition does not preclude clinicians from screening or counselling with regard to firearm safety.33
Counselling about Firearm Safety and Locked Storage
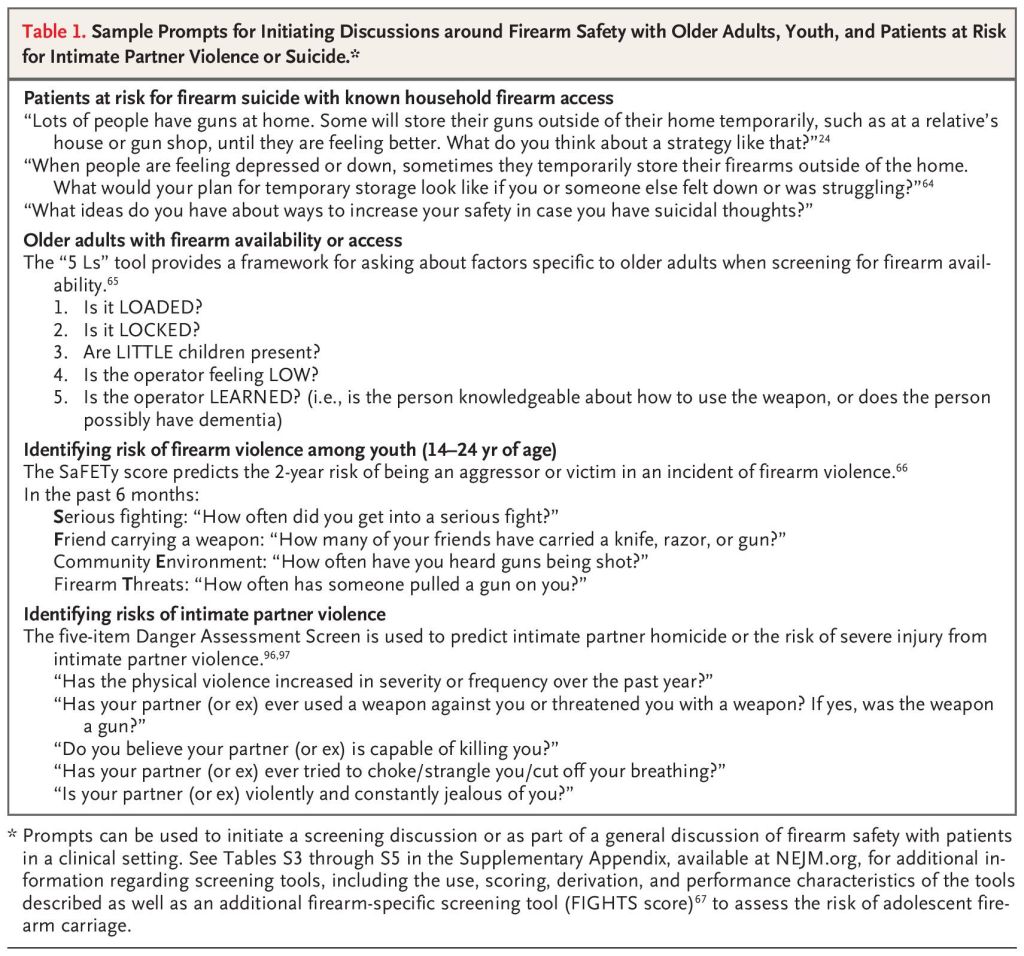
Validated clinical screening tools are available to help identify adolescents at risk for violent injury, violence perpetration, retaliatory violence after an assault with injury, firearm carriage, and firearm violence.66,67,89 Firearm-specific screening tools, such as the FiGHTS (Fighting, Gender, Hurt while fighting, Threatened, Smoker) and SaFETy (Serious fighting, Friend weapon-carrying, community Environment and firearm Threats) scales,66,67 were developed primarily as behavioral-health questionnaires for use among youth who are seen in urban emergency departments rather than in primary-care settings owing to lower primary-care attendance by late adolescence (Table 1).17,29,89 Prospective validation of these findings among broader samples or adaptation for other relevant (e.g., rural) contexts is needed.
Community Firearm-Related Violence: Youth Violence Prevention Counselling
First, most provide behavioural therapy28 or use trauma-informed approaches 89,90 that recognize that patients have substantial physiologic and psychological consequences from repeated exposure to violence. The “scared safe” approach (e.g., tours of a hospital trauma bay) used in earlier programs has been identified as harmful or ineffective and should be avoided.89,90
Second, most effective programs include a focus on retaliatory violence, using cognitive and behavioral therapy to enhance coping, anger management, violence avoidance, and nonviolent conflict-resolution skills to interrupt trajectories of violence.28,90
Third, programs address key risk factors (e.g., substance use and firearm carriage) while emphasizing promotive factors (e.g., prosocial peers and mentors) that enhance resilience.92
Fourth, several programs provide case management to help patients navigate medical, social, and psychological services.89,90 They also recognize a spectrum of dose intensities from single sessions28,29 for primary prevention to multiple sessions for youth further along a risk trajectory.
Sources & Credit;
Clinical Approaches to the Prevention of Firearm-Related Injury | New England Journal of Medicine https://share.google/G8Hn84Rff6ScUI1QD
https://unsplash.com/photos/a-black-and-white-shirt-with-a-graphic-design-on-it-QlmWhfMnXvY?utmsource=unsplash&utmmedium=referral&utmcontent=creditShareLink
