





We aimed to comprehensively evaluate the impact of ODA funding on mortality across the past two decades, and to project the potential consequences of current defunding trends.
We conducted an integrated retrospective evaluation and forecasting analysis using longitudinal panel data from 93 low-income and middle-income countries (LMICs). First, we estimated the association between ODA per-capita funding and mortality outcomes from 2002 to 2021 using a two-ways fixed-effects multivariable Poisson regression model with robust standard errors, adjusted for all relevant demographic, socioeconomic, and health-system covariates. We then assessed age-specific and cause-specific effects, performing extensive sensitivity and triangulation analyses to test the robustness and causal interpretation of results. Finally, we integrated the retrospective impact estimates into validated country-level microsimulation models to forecast mortality under three defunding scenarios up to 2030: a business-as-usual trajectory, a severe defunding scenario, and a mild defunding scenario.
In 1969, the Development Assistance Committee (DAC) of the Organization for Economic Cooperation and Development (OECD)—now composed of 38 high-income and upper-middle-income donor countries—introduced the concept of official development assistance (ODA) to standardise member governments’ aid to developing countries.1,2 In 1970, the General Assembly of the UN proposed that donor countries allocate 0·7% of their gross national product to ODA—a target that only a few countries have met to this day. ODA constitutes the core and most rigorously measured component of assistance, representing the majority of external financing for least-developed countries (LDCs). ODA flows consist of grants—which make up the largest share of ODA—and concessional loans provided to the official sectors of countries and territories on the DAC List of ODA recipients, as well as to international non-governmental organisations and multilateral development institutions.3
At a high level, ODA can be delivered bilaterally, from donor governments to recipient countries, or multilaterally to eligible multilateral organisations such as UN agencies and The Global Fund to Fight AIDS, Tuberculosis and Malaria, through technical cooperation or humanitarian assistance. To be counted as ODA, financial disbursements must meet criteria set by the OECD DAC. ODA does not include military aid, except for the cost of using armed forces to deliver humanitarian aid.
Higher ODA funding levels were associated with a 23% reduction in age-standardised all-cause mortality (rate ratio [RR] 0·77; 95% CI 0·70–0·85) and a 39% reduction in under-5 mortality (0·61; 0·49–0·75). ODA funding was associated with large mortality declines in major communicable diseases: 70% for HIV/AIDS (RR 0·30; 95% CI 0·24–0·39), 56% for malaria (0·44; 0·35–0·56), 56% for nutritional deficiencies (0·44; 0·30–0·65), and 54% for neglected tropical diseases (0·46; 0·36–0·59). Significant reductions were also observed in mortality from tuberculosis, diarrhoeal diseases, lower respiratory infections, and maternal and perinatal causes. Forecasting analyses projected that ongoing reductions in ODA funding could, under a severe defunding scenario, result in 22·6 million (95% uncertainty interval [UI] 16·3–29·3) additional deaths across all ages by 2030, including 5·4 million (4·1–6·8) among children younger than 5 years. Under a mild defunding scenario—defined as a continuation of current downward trends—the projected excess deaths would be 9·4 million (95% UI 6·2–12·6) overall and 2·5 million (1·8–3·2) among children younger than 5 years.
Our study design and analytical approach are the same as our recent study on the health impact of USAID defunding,6 and integrated two complementary components: a retrospective (ex-post) impact evaluation covering the period 2002–21 (more recent years were excluded due to sparse data availability across all variables), and a forecasting (ex-ante) analysis from 2025 to 2030. Both analyses were built upon a common data architecture, study design, and analytical framework to ensure methodological consistency and comparability.
The retrospective impact evaluation applied a longitudinal ecological design, in which countries served as the primary unit of analysis and were observed across multiple timepoints. This panel dataset incorporated aggregated demographic, socioeconomic, health, and ODA indicators compiled from multiple publicly available international sources (see appendix p 5 for full data details). The analytical sample comprised 93 LMICs, representing 6·3 billion individuals, selected from the global set of nations based on income classification criteria, data availability, and data consistency (see appendix p 6 for a detailed description of the country selection criteria). Models including all 130 LMICs with available data were also estimated as a sensitivity analysis (appendix p 31).
Study variables
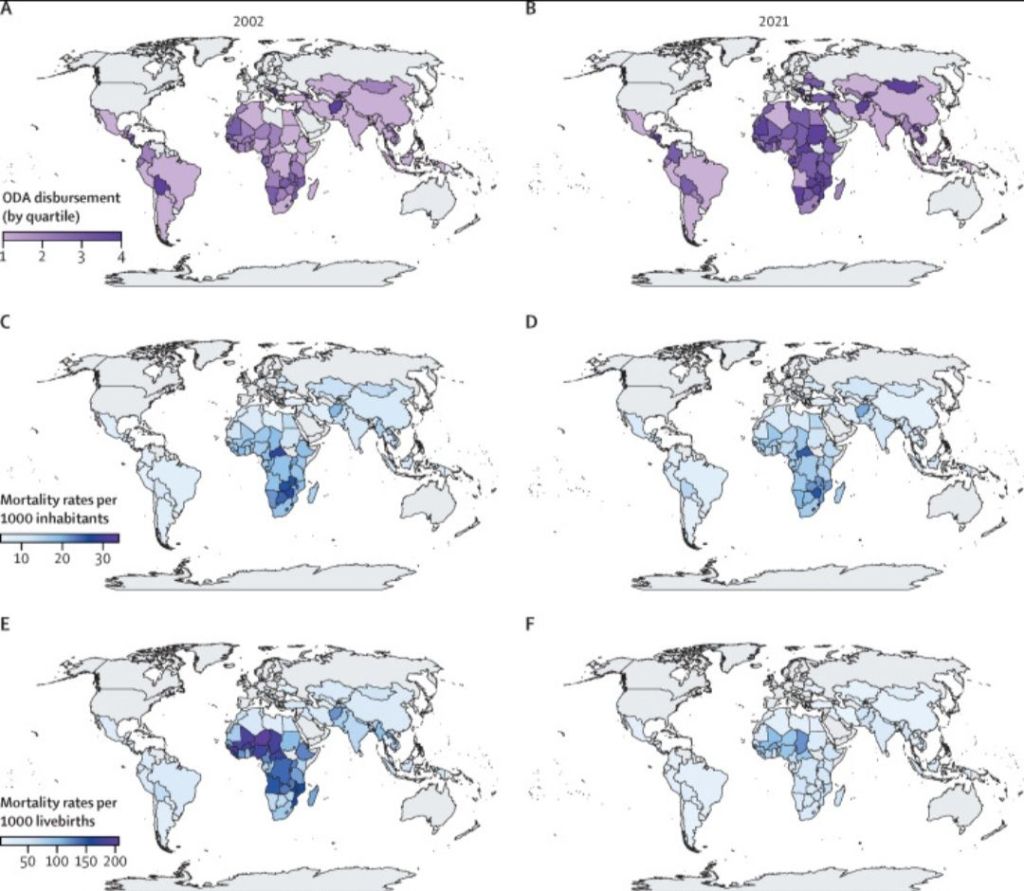
The main dependent variable in the analysis was the age-standardised all-cause mortality rate (ASMR) per 1000 inhabitants. Additionally, mortality was examined across different age groups, including within children younger than 1 year and those younger than 5 years (per 1000 livebirths). To examine cause-specific associations, we identified a set of mortality categories corresponding to ODA’s strategic health priorities and to conditions strongly associated with poverty, as informed by previous research.8–12 Each category was defined in accordance with ICD-10. The selected causes comprised tuberculosis (A15–A19 and B90), HIV/AIDS (B20–B24), maternal causes (O00–O99), lower respiratory infections (J09–J22, P23, and U04), malnutrition (E00–E02, E40–E46, E50, D50–D53, D64.9, and E51–E64), diarrhoeal diseases (A00, A01, A03, A04, and A06–A09), malaria (B50–B54, P37.3, and P37.4), and neglected tropical diseases (A66, A67, A69.1, A71, A77, A78, A79, B55–B56, B57, B65, B66, B73–B74, B76–B77, B79, B83, B88.0, and B88.1).
Our exposure variable was the financial assistance provided by OECD official donors in sectors encompassing determinants and interventions with plausible impacts on mortality. These included social infrastructure and services, covering education, health, population policies and reproductive health, water supply and sanitation, government and civil society, social protection, and housing policy; multi-sector and cross-cutting areas, such as general environmental protection, food security and safety, and disaster risk reduction; and humanitarian aid, including emergency response, reconstruction relief and rehabilitation, and disaster prevention and preparedness. Sectors with negligible effects on health in recipient countries—such as donors’ administrative costs, support for refugees in donor countries, and unspecified interventions—were excluded. The selected sectors represented approximately 55% of all ODA funding over the study period.
High levels of funding were associated with lower mortality, in particular a 23% reduction (rate ratio [RR] 0·77; 95% CI 0·70–0·85) for overall ASMR, 33% reduction (0·67; 0·55–0·82) for under-1 mortality, and 39% reduction (0·61; 0·49–0·75) for under-5 mortality. When causes of death in all-age mortality were analysed, high levels of ODA funding were associated with large mortality declines in major communicable diseases: 70% for HIV/AIDS (RR 0·30; 95% CI 0·24–0·39), 56% for malaria (0·44; 0·35–0·56), and 56% for nutritional deficiencies (0·44; 0·30–0·65), among others (table 3). In complementary stratified analyses (appendix pp 21–31), the associations between high levels of per-capita ODA funding and reductions in ASMR were stronger in low-income countries (29%) and lower-middle-income countries (25%) than in upper-middle-income countries and were more pronounced among women (27%) than among men (23%).
Extracted from The Lancet Global Health, Volume 14, Issue 5, May 2026

Leave a comment