





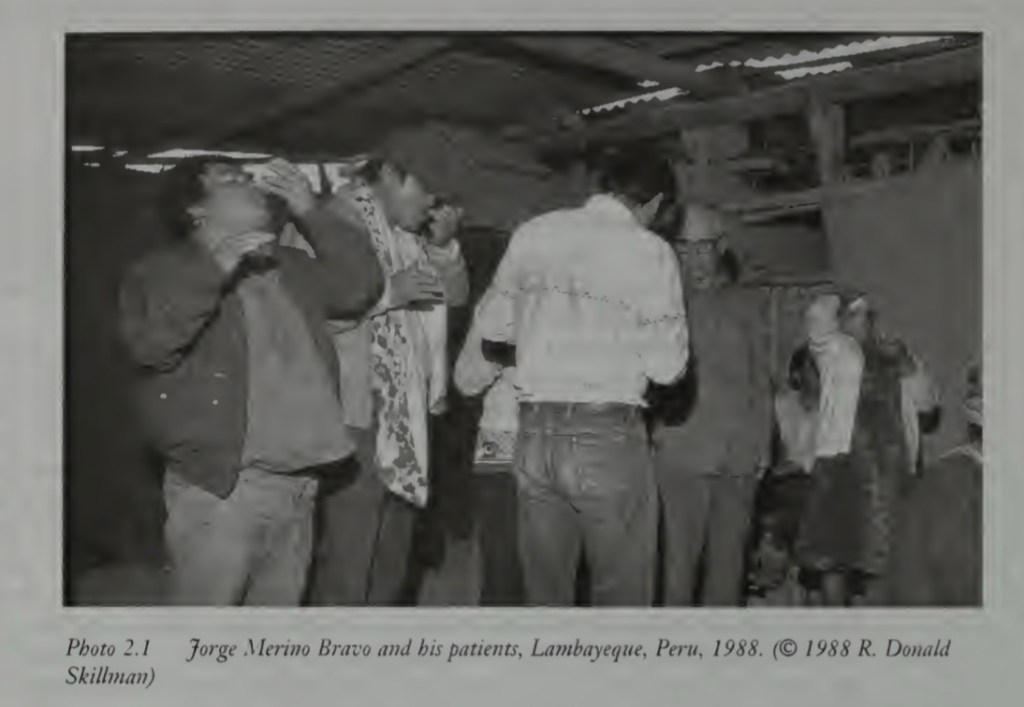
North coast of Peru, 1980: It’s three in the morning, the ocean breeze is wet and cold. It is not clear if my present nausea is attributable to the mescaline-bearing San Pedro (Trichocereus pachanoi) brew with which I began the evening or to the vile black-leaf tobacco sludge I have been asked to snort repeatedly. For the moment, the shaman’s rattling and chanting have stopped. In the partial light of the moon, I can see my fellow participants huddled under blankets up against the reed windbreak: some dose; others talk in in hushed voices. I hear one in the dune behind me, retching and coughing.

The shaman’s head is down, his gaze fixed on the objects arrayed in front of him. Two assistants sit with stools by his side. Nineteen adults and one ten-year-old boy have entrusted him with their care, hey expect him to learn the source of their suffering and to put things right. There are poor and middle-class men and women, some from close by and others from far away. A few have come alone, but most have spouses, friends and close family members at their side.

The shaman will tell most of them that their plans and incapacities, their bad fortune and sorrows, result from the injurious actions of envious neighbours, jealous competitors, or the illicit lovers of their mates. The label he will apply to their suffering is daño (“harm”), a sickness category linked to the malicious work of sorcerers. The shaman’s task is to cleanse each person of the sorcerer’s poisons and, in some cases, to reverse the harmful effects to punish the responsible party.
What are we to make of this event and of the diagnosis of daño? The ritual is certainly unlike the practices of medical practitioners with which we are more familiar. The idea of sorcery-induced illness brings with it negative associations built on Hollywood visions of voodoo ceremonies. It would only be in the spirit of cultural sensitivity that we would apply the term medical to the body of knowledge on which the Peruvian shaman depends on treating his clients; in unguarded moments, we might even be tempted to use less flattering adjectives, such as superstitious or primitive.
The assumption guiding our response to the Peruvian healing ceremony is that there are two kinds of knowledge about sickness, scientific and non-scientific. To diagnose a set of symptoms and organic manifestations as a viral infection, for example, is to use an objective, biologically based scientific concept. Naming a group of symptoms daño, however, is to apply a cultural category that has no scientific standing. What distinguishes contemporary biomedicine from healing traditions such as that described above is precisely that it is founded on scientific notions of disease that are supposedly free from any cultural content.
Applied Roots of Medical Anthropology
In the aftermath of World War II, the United States sought to extend its influence in the world via foreign assistance programs modelled on the successful Marshall Plan, which helped rebuild devastated Europe. Among the development projects supported by the International Cooperation Administration, precursor to the Agency for International Development (AID), and later by the United Nations’ World Health Organisation (WHO), were many that sought to eradicate epidemic diseases and improve basic sanitation in poor countries. Often, these public health campaigns foundered because of what the development specialists called “cultural obstacles”: resistance or opposition that seemed to relate to cultural misunderstandings between the developers and the “recipient peoples.” When this occurred, anthropologists were hired to identify and remove cultural impediments blocking the success of the projects.
An early example of anthropological work on international health projects was Richard N Adams’s (1955) analysis of village resistance in Guatemala to a child nutrition program supported by WHO and the Pan American Sanitary Bureau and directed by the Nutritional Institute of Central America and Panama (INCAP). Local ethnographic work revealed that community members interpreted INCAP as a communist organisation, a very serious assessment given the country’s right-wing ruling class and its violent anticommunism campaigns. They also considered the project’s requirement that children have blood samples taken as detrimental to their health. Guatemalan Indians believe that blood is a nonregenerative vital fluid, so the samples were seen as a permanent loss of strength. In addition, the idea that outsiders would wish to fatten up the children of the village was linked to popular mythology, dating back to the time of the conquest, in which whites capture Indian children to eat them. There were many good reasons, from the viewpoint of the villagers, to keep the children out of the program.
The involvement of anthropologists as cultural experts on international health campaigns directed new attention to disease and healing as subjects for anthropological analysis. The notion of an “applied anthropology in medicine” (Caudill 1953) predates the widespread use of the term medical anthropology, which indicates how central this work was to the development of a discrete anthropological subfield focused on medicine. One of the earliest collections of essays properly considered medical anthropology (Paul 1955) was a series of case studies of applied work in international and domestic public health projects. The first general literature review of medical anthropology (Scotch 1963) shows the pre ponderance of research directly related to international health projects. The application of anthropological theory and methods in both preventive and curative medicine still remains a core component of medical anthropology.
Medical Anthropology Today
In 1971, a “Society for Medical Anthropology” was formed under the administrative structure of the American Anthropological Association (AAA). By 2004, the society had 2,293 members, or about 12 percent of the total membership of the AAA; it is among the largest of the specialised societies in the organization. Over the past twenty-five years, major new journals and new sections of existing journals have appeared that are either completely or partly dedicated to the publication of research in medical anthropology: Medical Anthropology Quarterly, Medical Anthropology, Culture, Medicine and Psychiatry, Social Science and Medicine, and Ethnomedizin. Many major academic publishers now have specialized series in medical anthropology. In short, after a slow beginning, medical anthropology has caught on and now is among the most vibrant and productive subfields of the discipline.
As the earlier discussion suggests, part of what medical anthropologists do is to explore how sicknesses are “culturally constructed.” How a society’s understandings of and responses to diseases shaped by cultural assumptions about such things as the beginning and end of life, the workings of the human organism, and the causes of ill health and misfortune? The cultural-constructivist or interpretive approach to medical anthropology addresses this question. A second concentration in medical anthropology, the ecological or ecological/evolutionary approach, analyses the interaction between sociocultural patterns and the biological and environmental parameters within which humans operate. The approach draws on evolutionary theory and the concept of adaptation to explore the short- and long- term implications for human health of different environments and social and cultural arrangements. For example, what new patterns of disease accompanied the shift from hunting and gathering to sedentary agriculture in tropical regions? What were the short-term physiological and long-term (i.e., evolutionary) genetic consequences of this change in subsistence practices (Cohen 1989)?
Medical anthropologists have recently been challenged to pay more attention to the fundamental role that socioeconomic arrangements have on human health. Inspired by the literature in the political-economy of health and Marxist theory, critical medical anthropologists ask how the distribution of wealth and power and the division of labour affect disease patterns and healthcare access. Their role is most often that of a culture broker, an intermediary between biomedical practitioners and groups whose cultural assumptions might be at odds with those underlying scientific medicine. From programs sponsored by WHO to American hospitals serving ethnically diverse, applied medical anthropology pursues more effective health interventions.
The four currents in medical anthropology interpretive, ecological/evolutionary, critical and clinically applied, have had largely independent trajectories in the profession. The tendency for medical anthropologists to specialise in one approach has limited the opportunity for a cross-fertilisation of ideas. Paradoxically, it was the assault launched by critical medical anthropologists on all four perspectives (e.g., Singer 1989a) that initiated conversations about the possibility of an integrative approach to medical anthropology. A central objective of this text is to move closer to this integration, to develop an approach to the study of health and disease that (1) pays attention to ecological, biological, and cultural factors; (2) considers the political and economic forces that influence disease patterns and affect access to healthcare resources; and (3) offers an opportunity for health-promoting interventions.
[Basically, in simple lay man language epidemiologists ask what and where and a medical anthropologist asks why and how?]
Studying Shamans in Peru
Anthropological Questions and Methods in the Study of Sickness and Healing
Let’s return to the curing ritual that introduced the first chapter. Imagine that you have travelled to Peru to do research on this healing tradition. Imagine as well that little is known about these shamans and practices. What questions would seem important to answer? What areas of inquiry would you wish to explore? Just as important, how would you go about organising your research and gathering the information you consider essential?
Begin with the shaman himself. You might want to know something about his training, about what it takes to become a curandero, as these specialists are known in Peru. Perhaps your interest is in his curing knowledge: What distinctions does he make among types of sicknesses and how does he determine which a given patient has? What does he consider the source of his healing power? What botanical knowledge does he draw on his curing work? Is his healing based on spiritual assumptions and, if so, how do these relate to religious conceptions in the broader society?
Then there is the question of the use of drugs by the shaman, his assistants, and the patients. Does the San Pedro cactus, which bears mescaline at about the same concentration as peyote, trigger hallucinations for everyone who takes it? If so, how much of the content of these altered states is attributable to cultural expectations and how much to neurochemistry? If not, what other effect(s) does the drug have? (Keep in mind that it is used in combination with a liquefied tobacco juice imbibed through the nose.) Analysing the neurochemistry of mescaline without paying attention to what the shaman tells you about his therapeutic use of San Pedro would provide an incomplete understanding of the drug’s use. So far, we have barely mentioned the patients. You might wish to learn who they are and why they have come to a shaman to be cured. What are their educational and economic/class backgrounds? What symptoms are the patients experiencing and how they have interpreted them?
Of course, all these questions apply to a single shaman and his clients—how could you be sure that the answers relate as well to other shamans and their patients? Some kind of comparative work would be in order, with a sample of other specialists sufficient to represent the full range of curing practices. It would be important to establish a clear definition of what distinguishes curanderos from other who are also engaged in healing activities, as well as to document how all varieties of curers (medical doctors included) relate to one another (do MDs refer to curanderos?). Other aspects of the general context in which shamans work might also be of concern (e.g., legal statues governing medical practices and treatment of curanderos by state officials, costs of curandero treatments compared with other types of curers, knowledge among the general public of shamanic healing and of the reputations of specific shamans).
There is another dimension to this healing tradition that would also merit attention: its history. How long have shamans been a part of Peruvian culture and to what degree have their curing methods changed? Because contemporary Peru is a mix of Spanish, African, and native Andean cultures, you might even look for evidence of indigenous sources for the shaman’s work. This could involve searching for parallels in current Indian communities as well as for archaeological precedents. An exploration of early colonial documents might help to define the balance between Spanish and native cultural sources for shamanic practices, as well as the potential contribution from African slaves who were imported by the Spaniards soon after conquest.
Beth’s Review of Sorcery and Shamanism: Curanderos and Clients in Northern Peru by Donald Joralemon, Douglas Sharon
This remarkable ethnography explores a thriving tradition of urban shamanism. Peru’s northern coast is famous as a center of curanderismo, a folk healing system that blends popular Catholicism with indigenous symbolism. In midnight ceremonies held at backyard altars near cities like Trujillo and Chiclayo, mestizo shamans ingest mescaline brews of San Pedro cactus and perform songs, prayers and ritual cleansings. The setting will be familiar with anyone who has seen Sharon’s classic film, Eduardo the Healer (1978), about charismatic Eduardo Calderón, who is of 12 curers examined in this book.
Sorcery and Shamanism looks at how shamans and their clients use the discourses of sorcery and curing to cope with economic chaos and gender politics in contemporary Peru. Curanderos work by manipulating complementary forces of good and evil, right and left, up and down. Joralemon and Sharon structured their text around a similar dynamic of examining curanderismo from two distinct vantage points, reflected in the book’s two-part organization. Part 1, written mostly by Sharon, with contributions from Joralemon and Donald Skillman, focuses on shamans and the symbolism, metaphysics, and historical roots of their healing art. Part 2, written by Joralemon, looks at clients’ experiences and the social impact of curanderismo from the viewpoint of critical medical anthropology.
This is collaborative research at its best. The text builds on multiple shifts in perspective, moving between shamans and their patients, cosmology and political economy, shamanism as a belief system and shamanism as business. The result is one of the most comprehensive, richly nuanced studies in the ethnomedical literature.
Part 1 begins with short chapters on 12 curanderos’ life histories and ritual practices. This broad scope is a welcome counterweight to tendencies that have plagued shamanism studies since Eliade’s search for shamanic archetypes. Joralemon and Sharon explicitly reject reductionist approaches that represent ethnomedical beliefs as homogenous systems and exoticize shamans and ethereal metaphysicians. Instead, they emphasize differences in individual curanderos’ practices and show them as down-to-earth men (no female curers are included) concerned with bottom lines and business trips as well as spiritual journeys. Accounts of the authors’ relations with each shaman are woven through the text. They reveal the frustrations and unforeseen events of fieldwork and highlight the special problems and responsibilities that come with studying shamanism today.
While sometimes honoured as a national folkloric tradition, curanderismo is technically illegal in Peru. For centuries shamans have faced police harassment, arrests, and condemnation from church and civic officials. The curers in this study dealt with repression (and tried to get an edge on their shamanic competitors as well) by cultivating ties to people of higher standing and by adopting the trappings of pseudo-official status: business cards, framed documents, and consultation rooms like those of medical doctors. Increasingly, curanderos also came to see anthropologists as resources in their quest for legitimacy.
For years anthropologists have argued for recognizing the value of traditional medicine. This book explores what happens when that battle is partially won, though not exactly in the way academics had in mind.
In a provocative discussion of “the researcher effect,” Joralemon notes that academic attention has been “good for business” among curanderos (p. 163). In the 1980s, documentary films and media coverage of research on Peru’s folk healers conferred on them a new respectability, which was reinforced by the growing regard for traditional medicine in international health and development circles. As anthropologists’ work brought Eduardo Calderón international renown, he became a guru to New Age seekers from Europe and North America and adopted a new discourse of power animals, chakras, and planetary consciousness. His case illustrates the problem of defining “authenticity” in a world of permeable cultural boundaries, where today’s local healer may become next year’s talk show celebrity.
Incorporating foreign ideas and symbols is nothing new in Peruvian shamanism. Diverse cultural influences are evident in curers’ elaborate mesas (altars) composed of numerous ritual objects: pre-Columbian artifacts, Catholic icons, military swords, crystal balls, Amazonian rattles, Buddha statuettes. The dozen shamans’ mesas are analysed in more detail than most readers will want. Non specialists might skim these passages and turn to Sharon’s insightful synthesis, which suggests links between urban curanderismo and native Andean and Amazonian cosmologies.
In part 2 the focus shifts from shamans to their clients. The authors, assisted by a team of Peruvian and North American re-searchers, interviewed 129 individuals who consulted four of the curanderos. Case histories reveal the diverse problems that lead people to curanderismo and show how different shamans’ curing methods address patients’ feelings of being at risk.
Check out this video, “Eduardo the Healer” [WARNING: VIEWER DISCERTION IS ADVISED] (Cute guinea pigs were sacrificed in the film!)
https://share.google/MmchjKAdU1rUhzTo4
Sources:
Paragraph Bits Extracted from Exploring Medical Anthropology, Donald Joralemon
Reviewed Work: Sorcery and Shamanism: Curanderos and Clients in Northern Peru by Donald Joralemon, Douglas Sharon
Review by: Beth A Conklin
Medical Anthropology Quarterly

Leave a comment