





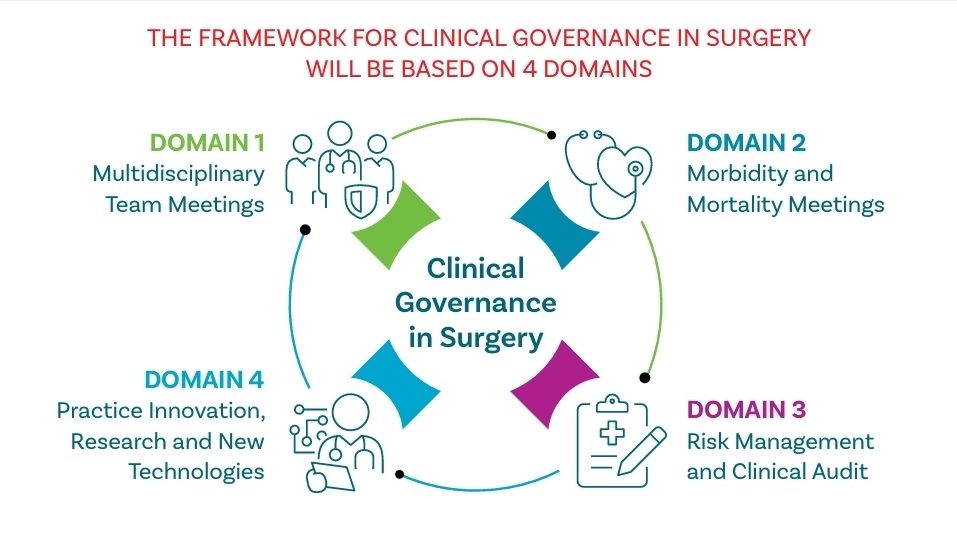
This year, the RCSI has released a Framework for Clinical Governance – a structured framework that could be used by surgical departments and healthcare departments to improve patient safety, clinical effectiveness, and professional accountability. Basically, it serves as a critical tool for ensuring excellence in surgical care.
This possibly cannot be overstated enough as it needs to done consistently and reliably! Effective governant structures means that there are well-established safety protocols and guidelines which reduce adverse events and improve the patient’s outcomes. Strong governance means that there is also a support system in place for the surgeons professional development and this includes the whole team as well – addressing workforce challenges and ensuring a high standards of practice sustainably.
This Surgical Clinical Governance Framework aligns closely with the Health Service Executive (HSE) Clinical Governance Framework which emphasises clear accountability, defined authority levels, patient safety, risk control, interdisciplinary collaboration, and continuous quality improvement. This Framework for Clinical Governance in Surgery which reflects international guidance as outlined by frameworks such as the Royal College of Surgeons of England’s (RCS Eng) “Good Surgical Practice” and the Royal Australasian College of Surgeons (RACS Australia) Clinical Governance Framework. RCSI has also produced an updated Code of Practice for Surgeons which outlines the professional standards to support our fellows and members in their day-to-day roles.
The objectives of the Framework for Clinical Governance in Surgery are to:
• Ensure patient safety through rigorous adherence to evidence-based surgical guidelines and practices.
• Foster accountability and clarity in clinical managerial roles within surgical departments.
• Promote continuous quality improvement through structured clinical audits and outcome analysis.
• Support robust incident reporting systems that facilitate learning from errors and near misses.
• Establish comprehensive evaluation and approval processes which foster innovation and research in surgical practices and technologies.
• Enhance communication, transparency, and trust among patients, healthcare providers and stakeholders.
• Provide comprehensive, ongoing professional development and training for all surgical personnel.
• Guide the implementation of clear mechanisms for monitoring, evaluating and refining governance practices regularly.

The framework is intended for use by:
• Surgeons and Surgical Trainees, to guide clinical practice and professional responsibilities.
• Regional Clinical Directors, Regional Clinical Leads, Clinical Directors and Perioperative Clinical Directors, for overseeing and ensuring compliance with governance standards.
• Hospital and healthcare system leadership, to implement policies and practices that support surgical governance.
• Healthcare policy makers and regulatory bodies, to inform policy development and ensure alignment with national and international healthcare standards.
• Members of surgical and peri-operative teams, including nurses, anaesthsiologists, and support staff, to ensure collaborative and coordinated care delivery.

Risk Management
• Clear and accessible inicident reporting systems aligned with the HSE Incident Management Framework.
• Incident reviews conducted transparently, following clear guidelines on open disclosure.
• Learning from incidents systematically integrated into clinical governance meetings, with clear feedback loops and accountability for implementing changes.
Clinical Audits
• Conducted regularly, with active participation from all surgical specialities and staff.
• Reviews adherence to relevant clinical standards and published best practices.
• Regular reporting of key surgical safety key performance indicators (KPIs) or metrics to be used and benchmarked, such as, but not limited to, Surgical Site Infection (SSI), Unplanned Returns to Theatre.
• Utlilises audit results to drive quality improvements, supported by adequate IT infrastructure for effective data tracking.
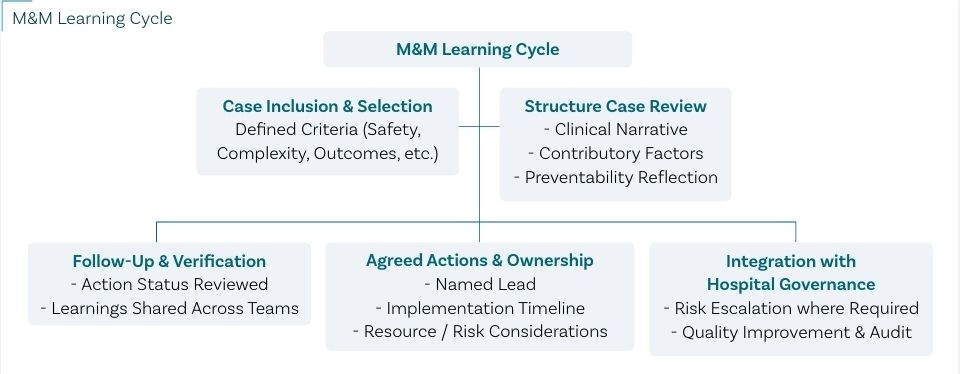
The importance of M&M meetings in surgical governance
Essential for fostering a culture of safety, accountability, and continuous learning within the surgical services;
a. Enhancing patient safety – By openly reviewing complications and adverse outcomes, teams can identify patterns, system failures or practice deviations that maybe contributing to harm, allowing for early interventions and preventive strategies
b. Supporting professional development – M&M meetings offer valuable educational moments for both trainees and consultants, reinforcing best practices and shared clinical wisdom
c. Fulfilling governance obligations – M&M processes align with national and insitutional frameworks for clinical management and quality assurance, such as the HSE’s Incident Management Framework
Active particiption in clinical audits for continuous performance review
• Encouragement of reflective practice to identify and rectify gaps in clinical care.
• Systematic training in new surgical techniques and technologies, such as robotic surgery, implantable devices and other minimally invasive methods, ensuring safe implementation and use.
• Ongoing educational sessions related to the latest clinical guidelines, patient safety protocols and governance frameworks.
• Training staff in recognising, reporting and reviewing incidents to learn and prevent recurrence integration of incident management training into regular professional development activities emphasising transparency and accountability.
Source and Credit – A Framework for Surgical Clinical Governance (RCSI) and RCSI Surgical Affairs

Leave a comment